| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Case Report
Volume 15, Number 2, April 2025, pages 64-67

Asymmetric Pre-Malar Swelling as an Unusual Presentation in a Case of Toxic Multinodular Goiter
Renaldo Pavreya, b ![]() , Shiksha Upadhyayaa, Keya
Baligaa
, Shiksha Upadhyayaa, Keya
Baligaa
aCentre for Accident & Emergency Medicine, Nanavati Max Super Specialty Hospital,
Mumbai, India
bCorresponding Author: Renaldo Pavrey, Centre for Accident &
Emergency Medicine, Nanavati Max Super Specialty Hospital, Mumbai, India
Manuscript submitted January 27, 2025, accepted March 20, 2025, published online April 29,
2025
Short title: Unusual Pre-Malar Swelling in TMNG
doi:
https://doi.org/10.14740/jem1503
| Abstract | ▴Top |
Toxic multinodular goiter (TMNG) and toxic adenoma are among the leading causes of thyrotoxicosis globally, with a rising incidence attributed to iodine-deficient regions. We report the case of a 34-year-old female who presented to the emergency department of our hospital with progressive unilateral facial swelling for 2 months, associated with squinting of the right eye. A thyroid function test revealed a thyroid-stimulating hormone (TSH) level of 0.007 mIU/L. Subsequently, a technetium-99 (Tc-99) thyroid scan revealed bilateral nodular lobes with heterogeneously increased trapping function, and a dominant hot nodule in the left lower pole, suggestive of TMNG. The patient was referred to an endocrinologist at our institute, and started on systemic carbimazole for 3 months. Her symptom improved progressively, and her TSH level increased to 2.18 mIU/L at the end of 3 months of initiating pharmacotherapy. This study explores the clinical presentation, diagnosis, and molecular pathogenesis of TMNG, including a study showing the association of asymmetrical pre-malar swelling with thyroid-associated orbitopathy (TAO), in some cases of TMNG. The diagnosis of TMNG is based on clinical signs, abnormal thyroid function tests, and imaging. However, more research is needed to establish the direct relationship between the pathophysiology of the development of asymmetric pre-malar swelling and TMNG. We conclude that asymmetric pre-malar swelling, as the first and only presentation of subclinical hyperthyroidism, is a rare but documented finding seen in patients with TMNG. We recommend that patients with asymmetric facial swelling be evaluated for thyroid abnormalities.
Keywords: Toxic multinodular goiter; Pre-malar swelling; Asymmetrical facial swelling; Thyrotoxicosis; Graves’ thyrotoxicosis
| Introduction | ▴Top |
Thyroid disorders are a common occurrence in India, especially among women [1, 2]. In an epidemiological study from the city of Kochi, in south-western India, subclinical hyperthyroidism was present in 1.6% of subjects participating in a community survey [3]. Subclinical hyperthyroidism is defined as a situation where the levels of the peripheral thyroid hormones are normal, but serum thyrotropin (TSH) is low [4]. Palpitations, tremors, heat intolerance, sweating, nervousness, anxiety, reduced feeling of well-being, fear, hostility, and inability to concentrate are some of the most common presentations of subclinical hyperthyroidism. Causes of subclinical hyperthyroidism may be endogenous (Graves’ disease, adenoma, multinodular goiter) or exogenous (excessive thyroid hormone replacement therapy) [5].
Toxic multinodular goiter (TMNG) and toxic adenoma account for a large proportion of thyrotoxicosis cases worldwide. With the ongoing improvement in iodine supplementation, particularly in developing countries, the incidence of TMNG is expected to rise. Research in molecular biology continues to provide insights into the genetic causes of TMNG, exploring how cellular abnormalities contribute to the development of autonomous thyroid nodules [6].
A patient could present with a neck bulge or deformity, an intolerance for tight necklaces, or an enlarging collar. Particularly in cases of big goiters, dysphagia, or breathing difficulties as a result of localized constriction of the esophagus or trachea may be evident [7]. Individuals could exhibit signs of hyperthyroidism, a condition whose clinical manifestation changes significantly with age. Classical signs of thyrotoxicosis, such as anxiety, losing weight despite increased appetite, palpitations, tremors, and heat intolerance, were more common in younger patients (≤ 50 years) in a series of 84 French patients with overt hyperthyroidism (42 patients), while anorexia and atrial fibrillation dominated in the older age group (≥ 70 years). Furthermore, older patients with TMNG are more likely to exhibit subclinical hyperthyroidism, which is characterized by low or suppressed TSH with normal free T4 and free T3 levels [7].
Asymmetric pre-malar swelling in TMNG is rare and under-reported. A study conducted between March 2002 and February 2005 reported that two out of six patients with TMNG presented with asymmetrical pre-malar swelling, a rare manifestation of thyroid-associated orbitopathy (TAO) [8]. Multinodular goiter involves both hyper- and hypo-functioning nodules; the overall enlargement of the thyroid and compression of nearby structures could contribute to facial edema, though the primary driving factor is usually the hyper-functioning nodules. We describe the case of a 36-year-old female who presented to us with the isolated symptom of progressive asymmetrical facial swelling over a period of 2 months.
| Case Report | ▴Top |
Investigations
A 34-year-old woman presented to the emergency department of a tertiary care private hospital in Mumbai, India, with progressive unilateral right-sided facial swelling for 2 months, as noticed by her family. This was associated with peri-orbital swelling, and mild squinting of the right eye. The patient had no other symptoms. There was no history of trauma, itching, redness, fever or pain. She denied palpitations, heat intolerance, weight loss or gain, anxiety, irritability, and depression; she also did not complain of neck swelling, dysphagia, or difficulty in breathing. The patient was pre-morbidly healthy, not on any regular medications, and her menstrual history did not reveal any dysfunctional bleeding.
On general examination, her vital signs were within the normal range, with no tachycardia or abnormal blood pressure. She was afebrile. Local examination did not reveal any tenderness around the facial swelling or any local rise of temperature. Systemic examination did not reveal any aberrant findings. There was no visible neck swelling or peripheral edema.
The following blood investigations were sent, which included a complete blood count (CBC), thyroid function test, and serum IgE levels. The patient was discharged from the emergency department, and was asked to follow up with the laboratory results.
On follow-up, her TSH level was 0.007 mIU/L (0.27 - 0.42 mIU/L), while free T3 and free T4 levels were within the normal ranges at 326 pg/dL (130 - 450 pg/dL) and 1.35 ng/dL (0.7 - 1.9 ng/dL), respectively, prompting us to a diagnosis of subclinical hyperthyroidism. Additionally, her hemoglobin was 8.1 g/dL, and IgE was 379.8 IU/mL. She was subsequently suggested to test for TSH-receptor antibody (TRAb) levels, and get a thyroid scan.
Diagnosis
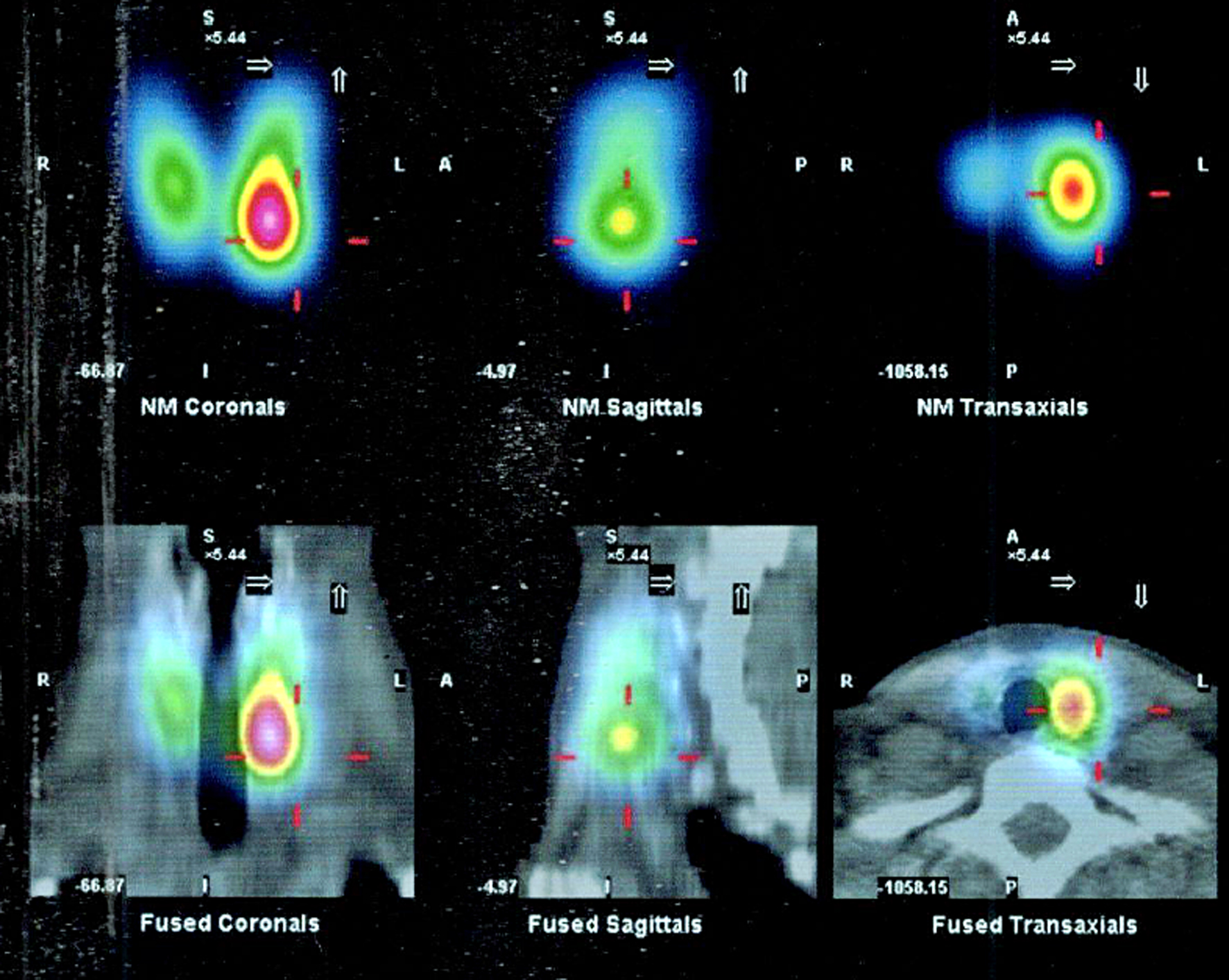
An expert consult was sought from our endocrinologist, who advised a technetium-99m thyroid scan; the TRAb test was deferred. The thyroid scan revealed bilateral nodular lobes, with heterogeneously increased trapping function and a dominant hot nodule in the left lower pole (Fig. 1) suggestive of TMNG.
 Click for large image |
Figure 1. SPECT-CT findings of multiple nodules in bilateral thyroid lobes with a dominant hot nodule involving the left lower pole (1.7 × 1.2 cm in axial dimensions). SPECT-CT: single photon emission computed tomography with computed tomography. |
Treatment
Therapy was initiated in the form of oral carbimazole at a dosage of 10 mg, twice daily for 2 months.
Follow-up and outcome
Two months later, there was visible reduction in the pre-malar swelling (Fig. 2). Repeat TSH level after 4 months was 2.18 mIU/L. Carbimazole has since been discontinued by the endocrinologist.
 Click for large image |
Figure 2. Follow-up at 2 months after initiating therapy showing a noticeable reduction in the right-sided pre-malar swelling. |
| Discussion | ▴Top |
Unilateral pre-malar or cheek swelling as an initial presentation of hyperthyroidism is not a common occurrence. A study conducted in Osmania General Hospital from 2012 to 2014 to study the cutaneous disorders associated with thyroid dysfunction found that facial swelling was seen as a common finding (31.25%) among the subgroup of patients with hypothyroidism, whereas the subgroup with hyperthyroidism commonly exhibited symptoms like swelling in the neck (65%), flushing (60%), pruritus (55%), and diffuse hair loss (40%) [9]. A systematic review done from 2013 to 2023, which included 108 papers (four randomized clinical trials, 21 systematic review or meta-analyses, 40 longitudinal prospective or retrospective observational studies, two cross-sectional studies, and 41 reviews) observed that subclinical hyperthyroidism is usually asymptomatic, or causes symptoms similar to but milder than those of overt hyperthyroidism [10].
This is not to say that facial swelling is an unheard of manifestation in hyperthyroidism. In fact, the most common extra-thyroidal manifestation of Graves’ disease is orbitopathy (25%), which can present as conjunctival erythema, periorbital edema (which our case study exhibits), lid retraction, and proptosis (which is contrary to the findings in our patient). Other extra-thyroidal Graves’ disease manifestations are pre-tibial myxedema which occurs in about 1.5% of patients, and acropachy (swelling in digits and nail clubbing) which occurs in about 0.3% [11]. A retrospective interventional case series from 2002 to 2005 revealed that in six patients (all female) among the 326 with TAO, TAO preceded the thyroid disease, or developed simultaneously [8]. The pre-malar and/or cheek swelling was bilateral in all cases, but two of the six were asymmetric. No diurnal fluctuation or tenderness in pre-malar and/or cheek swelling was noted. All improved incompletely over several months. Brow, eyelid swelling, and orbital-fat hypertrophy on radiological examination were coincidentally noted in five of six cases. Pretibial myxedema was noted in one case.
Thus, there is evidence that unilateral facial swelling can be seen as the only symptom of a thyroid disease, even though rare, and the patient must be evaluated for a thyroid disorder.
Learning points
Subclinical hyperthyroidism is difficult to diagnose due to the absence of overt symptoms, but more so when extra-thyroidal symptoms precede the thyroid disease. Thyroid disorders should always be a suspicion in patients with facial swelling (even unilateral). This helps in early recognition and treatment and can prevent long-term requirements of medication, as with our patient.
The incidence of TMNG may continue to decrease as global iodine supplementation improves. Accurate diagnosis relies on thyroid function tests, ultrasonography, and radionuclide scans. Emerging evidence links TMNG to rare presentations, such as asymmetrical pre-malar swelling associated with TAO. Further research into the molecular basis of TMNG may provide more targeted therapies and improve the management of this condition. More research needs to be done on the findings of asymmetric pre-malar swelling as a singular manifestation of TMNG.
Acknowledgments
None to declare.
Financial Disclosure
No funding was received for this work.
Conflict of Interest
The authors declare no conflict of interest regarding the publication of this paper.
Informed Consent
The authors of this article attest to the fact that informed consent has been acquired from the patient.
Author Contributions
Renaldo Pavrey: conceptualization, data curating, formal analysis, investigation, methodology, validation, writing - original draft, writing - review and editing. Shiksha Upadhyaya: data curating, formal analysis, writing - original draft. Keya Baliga: data curating, resources, writing - original draft.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
SPECT-CT: single photon emission computed tomography with computed tomography; TAO: thyroid-associated orbitopathy; Tc-99: technetium-99; TMNG: toxic multinodular goiter; TRAb: TSH receptor antibody; TSH: thyroid-stimulating hormone
| References | ▴Top |
- Unnikrishnan AG, Menon UV. Thyroid disorders in India: an
epidemiological perspective. Indian J Endocrinol Metab. 2011;15(Suppl
2):S78-81.
doi pubmed - Pearce EN. Diagnosis and management of thyrotoxicosis. BMJ.
2006;332(7554):1369-1373.
doi pubmed - Usha Menon V, Sundaram KR, Unnikrishnan AG, Jayakumar RV,
Nair V, Kumar H. High prevalence of undetected thyroid disorders in an iodine sufficient adult
south Indian population. J Indian Med Assoc. 2009;107(2):72-77.
pubmed - Koutras DA. Subclinical hyperthyroidism. Thyroid.
1999;9(3):311-315.
doi pubmed - Biondi B, Palmieri EA, Klain M, Schlumberger M, Filetti S,
Lombardi G. Subclinical hyperthyroidism: clinical features and treatment options.
Eur J Endocrinol. 2005;152(1):1-9.
doi pubmed - Siegel RD, Lee SL. Toxic nodular goiter. Toxic adenoma and
toxic multinodular goiter. Endocrinol Metab Clin North Am. 1998;27(1):151-168.
doi pubmed - Krohn K, Fuhrer D, Bayer Y, Eszlinger M, Brauer V, Neumann
S, Paschke R. Molecular pathogenesis of euthyroid and toxic multinodular goiter. Endocr Rev.
2005;26(4):504-524.
doi pubmed - Kim BJ, Kazim M. Prominent premalar and cheek swelling: a
sign of thyroid-associated orbitopathy. Ophthalmic Plast Reconstr Surg.
2006;22(6):457-460.
doi pubmed - Venkata KA, et al. A clinical study of cutaneous manifestations in patients with thyroid disorders. Journal of Evolution of Medical and Dental Sciences. 2016;5(74):5489.
- Lee SY, Pearce EN. Hyperthyroidism: a review. JAMA.
2023;330(15):1472-1483.
doi pubmed - Bartalena L, Fatourechi V. Extrathyroidal manifestations of
Graves' disease: a 2014 update. J Endocrinol Invest. 2014;37(8):691-700.
doi pubmed
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Endocrinology and Metabolism is published by Elmer Press Inc.