| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Case Report
Volume 15, Number 1, March 2025, pages 34-38

Pituitary Macroadenoma With Partial Transient Hypopituitarism
Pavel Stancheva, c, Ekaterina Babadzhanova-Hristovaa, c ![]() , Dimitar
Troeva, Boris Tilovb
, Dimitar
Troeva, Boris Tilovb
aClinic of Endocrinology and Metabolic Diseases, St George University Hospital,
Medical University of Plovdiv, Plovdiv, Bulgaria
bMedical College, Medical
University of Plovdiv, Plovdiv, Bulgaria
cCorresponding Author: Ekaterina
Babadzhanova-Hristova and Pavel Stanchev, Clinic of Endocrinology and Metabolic Diseases, St
George University Hospital, Medical University of Plovdiv, Plovdiv, Bulgariaand
Manuscript submitted November 26, 2024, accepted February 22, 2025, published online March 13,
2025
Short title: Pituitary Macroadenoma With Hypopituitarism
doi:
https://doi.org/10.14740/jem1052
| Abstract | ▴Top |
Pituitary tumors are lesions of the central nervous system that are usually benign and most often develop sporadically. Non-functioning pituitary adenomas range from being clinically asymptomatic to causing significant hypothalamic/pituitary dysfunction, including hypopituitarism, and visual field loss due to their large size. Pituitary macroadenomas (size over 10 mm) may cause elevated prolactin levels (“pseudoprolactinoma”) as a result of the lost dopaminergic inhibition on pituitary lactotrophs. Spontaneous recovery of the pituitary function in patients with hypopituitarism after surgical removal of a macroadenoma is rare. We present a clinical case of a 40-year-old man, referred for diagnostic clarification in a specialized endocrine clinic, due to easy fatigue and swelling of the lower limbs and outpatient-acquired data on secondary hypothyroidism. From the conducted complex hormonal evaluation, the patient presented with partial hypopituitarism (secondary hypogonadism and hypothyroidism) and hyperprolactinemia. The performed magnetic resonance imaging (MRI) of the brain revealed a pituitary macroadenoma, measuring 24 × 23 × 22 mm, without involvement of the optic nerves. After the execution of transsphenoidal adenomectomy, the patient underwent recovery of the pituitary function and did not require permanent hormone replacement therapy. The described clinical case provides evidence of the unique high reparative and regenerative potential of the pituitary gland that should be kept in mind during the follow-up period of patients with postoperative hypopituitarism.
Keywords: Transient hypopituitarism; Pituitary macroadenoma; Pseudoprolactinoma; Regeneration of the pituitary gland; Transsphenoidal adenomectomy
| Introduction | ▴Top |
Pituitary adenomas are a diverse group of benign tumors originating from the hypophysis. Depending on their size, they are classified as microadenomas (up to 10 mm) and macroadenomas (over 10 mm). After the introduction of electron microscopy and immunohistochemistry, the classification of pituitary adenomas was expanded [1]: they are now classified according to their hormonal activity as hormonally active (functioning) and hormonally inactive (non-functioning) [2]. Pituitary adenomas represent about 10-15% of all intracranial tumors [3].
An analysis by Fernandez et al showed that pituitary adenomas were more common in women (66.7%) than in men (33.3%), with functionally inactive ones being found predominantly in men. Their study also showed a frequency of 58.7% of microadenomas, compared to 41.3% for macroadenomas [4].
Patients with non-functioning pituitary adenoma (NFPA) generally have no clinical symptoms caused by elevated hormone levels, so that the condition is often neglected by patients or misdiagnosed by doctors, leading to the development of macroadenomas at the time of diagnosis. Most NFPAs are characterized by headache, visual disturbances, and hypofunction of the anterior pituitary, commonly due to slow, progressive enlargement of tumors or abrupt pituitary apoplexy [5, 6]. Tumor size and maximum tumor diameter are positively correlated with the incidence and degree of hypopituitarism. For patients with NFPA, anterior pituitary function should be examined after surgery in order to substitute the existing hormonal deficiencies and to monitor the occurrence of possible restoration of pituitary function [5, 6].
The presented clinical case is an example of the importance of monitoring and avoiding unnecessary therapy and polypharmacy in patients followed up after transsphenoidal adenomectomy for pseudoprolactinoma in connection with the high regenerative potential of the pituitary gland.
| Case Report | ▴Top |
Investigations
A 40-year-old male patient presented to the Clinic of Endocrinology and Metabolic Diseases with a history of childhood obesity, and unsuccessful attempts at weight reduction, despite his efforts to make a change in his diet and exercise regimen for the last 6 months. He reported complaints of easy fatigue and swelling in the lower legs. The patient had performed a consultation with a cardiologist on an outpatient basis and had been diagnosed with obstructive sleep apnea, so continuous positive airway pressure (CPAP) therapy had been started at night. Outpatient hormonal tests showed data for secondary hypothyroidism. The patient was referred to our specialized endocrine clinic for diagnostic clarification.
The obtained family history showed predisposition for type 2 diabetes and arterial hypertension. Due to chronic venous insufficiency of the extremities as a comorbidity, the patient was taking a venotonic, containing hesperidin and diosmin.
Diagnosis
Physical examination showed no skin abnormalities. The habitus was hypersthenic. Height was 180 cm, weight was 155 kg, and body mass index (BMI) was 47.8 kg/m2. Bilateral vesicular breath was noted, without wheezing. Rhythmic heart activity with a frequency of 78 - 80 beats/min and an arterial pressure of 130/80 mm Hg were recorded. No heart murmurs were detected by auscultation. Abdomen was soft, painless, with physiological peristalsis. Liver and spleen were not palpable. Limbs showed swelling in the lower legs and varicose changes.
The conducted basic blood tests (Table 1) showed normal blood count, ionogram, and kidney function. The hormonal evaluation provided data for secondary hypothyroidism and hypogonadism with elevated serum prolactin. The results from thyroid autoantibodies - anti-thyroid microsomal peroxidase antibody (anti-TPO-ab) and anti-thyroglobulin antibody (anti-Tg-Ab) - were within normal limits.
 Click to view |
Table 1. Basic Investigations |
Partial hypopituitarism was observed and the patient was started on a substitutional therapy with levothyroxine at 75 µg.
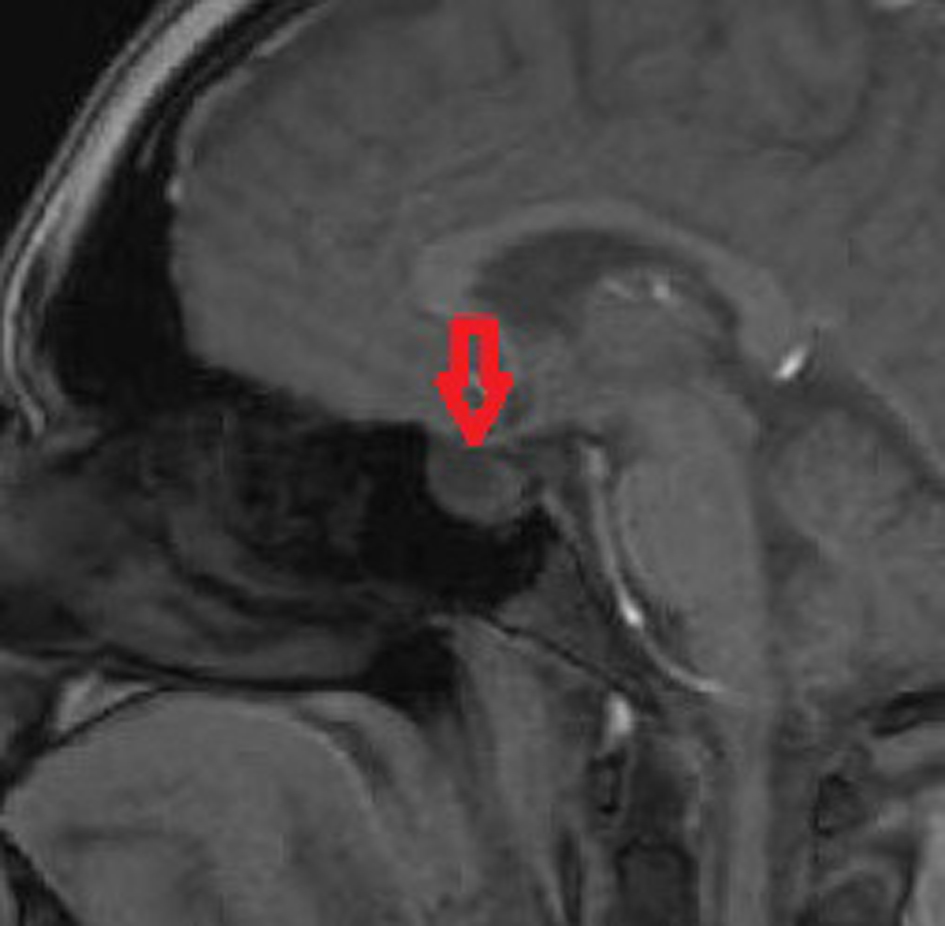
Magnetic resonance imaging (MRI) of the brain was performed due to the suspicion of a space-occupying process in the pituitary area. The MRI showed the following finding (Fig. 1): presence of a large, homogeneous, rounded median mass with a “snowman” shape in the pituitary region, originating from the sella, protruding upwards, lifting and compressing the optic chiasm and the overlying third ventricle. The formation involved the entire pituitary and measured 24 × 23 × 22 mm. The tumor expanded the sella turcica and extended towards the suprasellar cistern, lifting and slightly displacing the optic chiasm and the anterior floor of the third ventricle. It compressed the floor of the sella with protrusion towards the sphenoidal sinus. The gland and infundibulum were strongly displaced to the left. After intravenous contrast agent administration, delayed moderate contrast enhancement was observed in the solid parts of the tumor mass. Lateral expansion of the tumor in the cavernous sinus displaced the empty carotid flow laterally, enclosing the flow gap, which indicated the presence of vascular enhancement, without causing arterial constriction or occlusion, in contrast to meningioma. In the upper part of the lesion, there were no signal foci. In ventricular system, basal cisterns were located medially with relatively preserved symmetry and border dimensions. MRI angiography was performed and it showed normally presented vessels and preserved blood flow. No evidence of aneurysmal dilatations was found and the paranasal cavities were clear. Conclusion of the MRI data showed tumor process in the sella turcica with signs of pituitary macroadenoma and intraparenchymal hemorrhage in the tumor.
 Click for large image |
Figure 1. MRI of the brain showing tumor process in the sella turcica with signs of pituitary macroadenoma (sagittal plane). The arrow indicates the tumor mass. MRI: magnetic resonance imaging. |
Based on the conducted studies, the presence of a hormonally inactive macroadenoma - pseudoprolactinoma - was discussed. Pseudoprolactinoma is a tumor that does not secrete prolactin itself. The pseudoprolactinoma interrupts the flow of prolactin inhibiting factor, dopamine, from the hypothalamus through the pituitary stalk to the normal pituitary. The differentiation between prolactinoma and pseudoprolactinoma is vitally important since prolactinomas most commonly respond well in terms of tumor shrinkage to medical treatment using dopamine agonist therapy, whereas pseudoprolactinomas do not. Thus, surgical treatment is clearly indicated as first-line treatment in cases of pseudoprolactinoma [7].
Our patient was referred for consultation with a neurosurgeon, and subsequent surgical intervention of endonasal transsphenoidal biportal craniotomy was performed with adenomectomy.
Follow-up and outcomes
The patient had no complications in the postoperative period. Histological evaluation showed data for mixed cell pituitary adenoma.
After 2 months, a control MRI of the pituitary was performed (Fig. 2). The follow-up postoperative MRI showed no evidence of recurrence or residual tumor mass in the pituitary gland. “Empty sella” was found, without any current data on pathological changes in the brain.
 Click for large image |
Figure 2. Follow-up postoperative MRI of the brain. No evidence of recurrence or residual tumor mass in the pituitary gland was found. “Empty sella” was found, without any current data on pathological changes in the brain (sagittal plane). The arrow indicates the pituitary region. MRI: magnetic resonance imaging. |
The patient underwent an evaluation by a clinical psychologist, establishing significant psycho-emotional disorders. During the psychological evaluation, chronic anxiety and depressive symptoms were identified, characterized by constant fatigue, loss of interest in usual activities, and pronounced anxiety about his health. The patient reported frequent mood swings, expressed in irritability and apathy without an apparent external cause. Cognitive difficulties with concentration and short-term memory were also identified on performing daily tasks. The psycho-emotional symptoms, combined with apathy, further limited the patient’s social and professional activity, which required targeted psychological support and monitoring as part of the overall therapeutic plan.
The hormonal results of the patient during the first hospitalization and the follow-up period are presented in Table 2.
Click to view |
Table 2. Hormonal Results During the First
Hospitalization and the Follow-Up Period |
The presented clinical case is an example of a diagnosed pituitary macroadenoma (hormonally inactive pseudoprolactinoma) with partial transient hypopituitarism. In differential diagnosis, we discussed the presence of macroprolactinoma, but due to the lack of clinical manifestation, the improvement and lack of relapse after surgical treatment, the presence of hormonally inactive macroadenoma with the presence of hyperprolactinemia due to the impaired dopamine inhibition was rather assumed.
A tendency towards normalization of serum testosterone levels is noticeable postoperatively and a transient nature of the functional disorders of the pituitary gland has been observed. No testosterone treatment was administered before and after the surgical intervention. The dosage of the levothyroxine preparation was gradually reduced in therapeutic terms. During the follow-up, normal levels of thyroid-stimulating hormone (TSH), free thyroxine (FT4), and free triiodothyronine (FT3) were registered, and euthyroid state was observed 45 days after discontinuation of the levothyroxine preparation (Table 2).
Stimulation tests for evaluation of the functional capacity of the pituitary gland have not been performed at this stage. In the future, an assessment of the patient’s reproductive capacity is pending. In connection with the pronounced obesity and the lack of carbohydrate disorders, therapy with a glucagon-like peptide-1 (GLP-1) analogue with good gastrointestinal tolerance and initial effect on body weight was started. The patient remained on continuous monitoring of his hormonal results.
| Discussion | ▴Top |
According to the performed literature review, other clinical cases of transient functional impairment of the pituitary gland in the presence of an organic cause have been described. Noto and associates described a clinical case of a 50-year-old man with complaints of fatigue, loss of appetite, intolerance to low temperatures, and decreased libido. The hormonal tests showed evidence of hypopituitarism, and the MRI revealed data indicating the presence of lymphocytic hypophysitis. The patient was started on treatment with hydrocortisone and a levothyroxine preparation with a following improvement in his general condition. During the follow-up, the replacement therapy was gradually reduced and discontinued, and normalization of pituitary function was established [8].
Wende and associates described a case of a 60-year-old woman with an aneurysm of the right internal carotid artery protruding into the sellar region diagnosed on the occasion of a headache. Endovascular treatment of the aneurysm was performed. After the intervention, there was evidence of transient partial hypopituitarism [9].
Specific cell types, including gonadotropes and lactotropes, can undergo turnover during normal physiological processes, such as reproductive cycles and lactation. Several studies support the existence of multipotent stem cells in the adult pituitary from fish to human [10] and raise the question of their use as a substitute for a pituitary cell population, which still remains speculative. Clinical management of pituitary dysfunction, particularly following surgical interventions or injury, in most cases involves hormonal replacement therapy to compensate the lost endocrine function.
Conclusions
The presented clinical case is of great importance due to its emphasis on the presence of possible transience of the partial hypopituitarism in patients with NFPAs after surgery, which proves the large regenerative potential of the pituitary tissue. The reversibility should be taken into account by clinicians in order to avoid polypharmacy and adherence to unnecessary medications. The described case is yet another proof of the importance of the good communication between the medical doctor and the patient during the strict follow-up.
Learning points
The clinical case confirms the regenerative potential of the pituitary gland, even in the presence of an organic cause for the developed hypopituitarism. The article provides information for the necessary tests that should be performed pre- and postoperatively in patients with non-functioning pituitary macroadenomas, which could help the clinicians to prove the transient nature of the functional disorders during the follow-up of their patients.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
All appropriate consent forms were obtained from the patient for the publication of the case report. Consent was also given for images and other clinical information to be reported in the journal.
Author Contributions
Pavel Stanchev: concept, literature search, data acquisition, and manuscript preparation. Ekaterina Babadzhanova-Hristova: design, literature search, manuscript editing, and manuscript review. Boris Tilov: drafting of the manuscript and manuscript editing. Dimitar Troev: supervision and manuscript review. All authors have reviewed the final version to be published and agreed to be accountable for all aspects of the work.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
ACTH: adrenocorticotropic hormone; anti-Tg-Ab: anti-thyroglobulin antibody; anti-TPO-Ab: anti-thyroid peroxidase antibody; CPAP: continuous positive airway pressure; FT4: free thyroxine; FT3: free triiodothyronine; LH: luteinizing hormone; FSH: follicle-stimulating hormone; GH: growth hormone; MRI: magnetic resonance imaging; NFPA: non-functioning pituitary adenoma; TSH: thyroid-stimulating hormone
| References | ▴Top |
- Asa SL. Tumors of the pituitary gland. In: Rosai J, editor. Atlas of tumor pathology. 3rd series Fascicle 22. Washington, DC: Armed Forces Institute of Pathology; 1998. p. 1-214.
- Asa SL, Ezzat S. The pathogenesis of pituitary tumours. Nat
Rev Cancer. 2002;2(11):836-849.
doi pubmed - Lake MG, Krook LS, Cruz SV. Pituitary adenomas: an overview.
Am Fam Physician. 2013;88(5):319-327.
pubmed - Fernandez A, Karavitaki N, Wass JA. Prevalence of pituitary
adenomas: a community-based, cross-sectional study in Banbury (Oxfordshire, UK). Clin Endocrinol
(Oxf). 2010;72(3):377-382.
doi pubmed - Zhang R, Wang Z, Gao L, Guo X, Feng C, Deng K, Lian W, et
al. Clinical characteristics and postoperative recovery of hypopituitarism in patients with
nonfunctional pituitary adenoma. World Neurosurg. 2019;126:e1183-e1189.
doi pubmed - Tampourlou M, Fountas A, Ntali G, Karavitaki N. Mortality in
patients with non-functioning pituitary adenoma. Pituitary. 2018;21(2):203-207.
doi pubmed pmc - Jo JW, Lee EJ, Nam MS, Nam SY, Song YD, Lee HC, Huh KB, et al. Clinical and endocrinologic differences between prolactinoma and pseudoprolactinoma proven by immunohistochemical study. Endocrinol Metab. 1995;10(4):362-369.
- Noto H, Tsukamoto K, Hayashi S, Takano K, Fujita T, Kimura
S. Spontaneous recovery from hypopituitarism in a man with lymphocytic hypophysitis: a case
report. Endocr J. 2001;48(4):483-486.
doi pubmed - Wende T, Hamerla G, Quaschling U, Haase A, Meixensberger J,
Nestler U. Persistent hyperprolactinemia, transient hypopituitarism, and transient contralateral
third nerve palsy after endovascular treatment of an internal carotid artery aneurysm: case
report and review of the literature. SAGE Open Med Case Rep. 2020;8:2050313X20948714.
doi pubmed pmc - Camilletti MA, Martinez Mayer J, Vishnopolska SA,
Perez-Millan MI. From pituitary stem cell differentiation to regenerative medicine. Front
Endocrinol (Lausanne). 2021;11:614999.
doi pubmed pmc
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Endocrinology and Metabolism is published by Elmer Press Inc.