| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Original Article
Volume 15, Number 3, August 2025, pages 109-117

Exercise Perceptions in People With Metabolic Dysfunction-Associated Steatotic Liver Disease: Insights From a Qualitative Study
Kedar Deshpandea, f, John Olynykb, c, Oyekoya Ayonrindeb, c, d, e, Kazunori Nosakaa, e
aSchool of Medical and Health Sciences, Edith Cowan University, Joondalup, WA,
Australia
bCurtin Medical School, Curtin University, Perth,
Australia
cDepartment of Gastroenterology and Hepatology, Fiona Stanley
Hospital, Perth, Australia
dMedical School, The University of Western Australia,
Perth, Australia
eThese authors contributed equally to this
article.
fCorresponding Author: Kedar Deshpande, School of Medical and Health
Sciences, Edith Cowan University, Joondalup, WA 6027, Australia
Manuscript submitted May 9, 2025, accepted July 8, 2025, published online August 7,
2025
Short title: Exercise for MASLD Patients
doi: https://doi.org/10.14740/jem1527
| Abstract | ▴Top |
Background: Metabolic dysfunction-associated steatotic liver disease (MASLD) is a chronic liver condition associated with lifestyle and metabolic risk factors. While exercise is a beneficial treatment strategy, many patients struggle to implement and perform exercise regularly. It is important for practitioners to know about patient awareness, attitudes, and preferences regarding exercise in the context of MASLD. In this study, we examined exercise knowledge, attitudes, and exercise preferences among patients with MASLD to improve their exercise behavior changes.
Methods: We conducted a questionnaire and semi-structured interview study in adults with MASLD to assess their disease awareness, perspectives on exercise and exercise preferences. MASLD severity was assessed using controlled attenuation parameter (CAP) and transient elastography (TE) to determine the severity of hepatic steatosis and fibrosis, respectively. Transcripts were coded using NVivo software, and thematic analysis was employed to extract key themes.
Results: A total of 18 interviews were completed with 18 MASLD patients (37 - 76 years), who attended an outpatient hepatology clinic. The majority of participants demonstrated awareness of MASLD’s severity but lacked knowledge about exercise as a treatment option. Participants expressed preferences for exercises that were time-efficient, easy to perform, non-strenuous, and portable. Walking emerged as the most favored exercise, followed by resistance exercises with free weights and eccentric-biased bodyweight exercises.
Conclusions: This study provides insights into individuals’ perspectives on exercise in MASLD, highlighting the need for targeted education and personalized exercise interventions. Understanding these perspectives can inform the development of effective strategies to promote long-term exercise adherence and improve clinical outcomes in MASLD management.
Keywords: Exercise preferences; Patient awareness; Behavioral change; Portable exercises; Thematic analysis; Qualitative research
| Introduction | ▴Top |
The field around fatty liver disease has had several developments in the last some years. One of the most significant developments was the recent update in its nomenclature [1]. Metabolic dysfunction-associated steatotic liver disease (MASLD) was introduced as the new term to describe the condition instead of non-alcoholic fatty liver disease (NAFLD) [2]. Basically, both MASLD and NAFLD refer to the same disease [2, 3], thus we extrapolate previous findings regarding NAFLD to represent MASLD.
MASLD is the most common chronic liver disease, affecting approximately 30% of people worldwide [1, 2]. It is a chronic progressive disease that typically begins with steatosis and advances to metabolic dysfunction-associated steatohepatitis (MASH), characterized by inflammation and hepatocyte cell ballooning, in approximately 20-30% of the individuals. Some of these cases are at higher risk of developing liver cirrhosis and hepatocellular carcinoma [3]. MASLD is a major public health concern in Australia and worldwide, with the prevalent MASLD and MASH projected to increase by 25% and 40%, respectively, between 2019 and 2030 in Australia [4]. Adams et al [4] projected that there would be an 85% rise in the incidence of advanced liver disease and MASLD-related mortality by 2030 [4]. Furthermore, a recent study in a regional part of Australia found a 10% increase in MASLD prevalence over the last 15 years, particularly among women. Moreover, a considerable number of these people are at risk of developing liver fibrosis [5].
Currently, there is no approved pharmacological therapy for MASLD. Lifestyle interventions, such as regular exercise and dietary management, are the most important tools to reduce liver fat and potentially reduce the risk of future liver and cardiometabolic complications [6]. Regular exercise reduces hepatic fat content and improves insulin sensitivity, inhibits lipolysis in the fat cells and resulting in a reduced delivery of free fatty acids into the liver [6]. Furthermore, regular structured exercise also reduces the burden of extrahepatic comorbidities such as diabetes, obesity, cardiovascular disease, and cancer [7, 8].
Individuals with MASLD are recommended to achieve at least 150 - 200 min of moderate-intensity exercise per week, according to guidelines laid out by the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD) [9]. A systematic review of several exercise trials has concluded that both aerobic and resistance exercise are effective for reducing liver fat in individuals with MASLD [10]. The authors concluded that resistance exercise might be more favorable than aerobic exercise for patients with MASLD and poor cardiorespiratory fitness levels, as the intensity and energy expenditure associated with resistance exercises is significantly lower [10]. Hallsworth et al [11] suggested that an exercise modality personalized to the individual patient’s disease severity, comorbidities, fitness levels, and preferences would be the most effective in MASLD therapy.
Despite evidence showing that exercise can significantly reduce hepatic fat content, the majority of patients struggle to initiate and maintain good exercise habits [12]. A few studies reported that fatigue, lack of energy, prior injuries, lack of education and resources, and time constraints were the main barriers to exercise in individuals with MASLD [12, 13]. A potential explanation for fatigue and lack of energy may include the fact that individuals with MASLD often exhibit low levels of cardiorespiratory fitness levels, making exercise challenging [14, 15]. Another possible reason for lack of energy is the disturbance in energy metabolism resulting from mitochondrial dysfunction, which is highly prevalent in advanced MASLD. Consequently, there is reduced availability of energy for skeletal muscles to engage in exercise [16].
While a few studies have investigated the barriers and facilitators of exercise in individuals with MASLD [17, 18], there is a significant gap in behavioral research to address the attitudes and behaviors regarding exercise in individuals with MASLD. Therefore, the aim of the present study was to identify the type of exercises that individuals with MASLD would prefer to engage in and understand their perceptions that drive these choices with a combination of quantitative surveys and qualitative one-on-one interviews. We believe that this information can provide the groundwork for large-scale intervention studies to evaluate the efficacy of exercises chosen by individuals with MASLD as their preferred choices. These data could help address the gap in MASLD therapy by empowering healthcare practitioners with an effective and actionable exercise program for their patients.
| Materials and Methods | ▴Top |
Study population
We recruited adults attending an outpatient hepatology clinic at a tertiary Australian hospital with a clinical diagnosis of MASLD or MASH based on FibroScan® 502 Touch. Participants with a controlled attenuation parameter (CAP) score of ≥ 275 dB/m, consistent with the approved threshold for hepatic steatosis diagnosis, were invited to participate in the study. We characterized MASLD as a liver with steatosis accompanied by at least one metabolic risk factor, excluding excessive alcohol consumption, in accordance with the most recent consensus nomenclature [19]. Participants with secondary causes of chronic liver disease such as autoimmune hepatitis, viral hepatitis or significant alcohol consumption were excluded. Additionally, those with decompensated chronic liver disease presenting with hepatic encephalopathy, ascites, esophageal varices, and hepatocellular carcinoma were not included. Ethics approval was obtained from the Human Research Ethics Committee at South Metropolitan Health Service (SMHS) in Perth and Edith Cowan University. This study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration.
Study design
We designed a presentation for the participants with general information on MASLD and the role of exercise in management and treatment of this disease. We filmed a video demonstrating different types of exercises that can be performed for health optimization. We also included information about the recommended frequency and duration of these exercises and the correct technique to perform these exercises. Table 1 shows the types of exercises that were shown in the video. The exercise types were chosen based on previous studies showing effectiveness in improving health-related outcomes in humans [10, 20, 21]. We asked the participants to choose their top two exercises that they would prefer to perform regularly by ranking them 1 and 2 in questionnaire 1. We did this to understand the type of exercises that would be ideal for people with MASLD, since they generally show compromised cardiorespiratory fitness levels, with limited tolerance to exercise negatively affecting their ability and willingness to engage in regular exercise [22].
 Click to view |
Table 1. Types of Exercises That Were Shown to
the Participants in the Videos |
Eccentric exercise consists of mainly eccentric (lengthening muscle) contractions, in which activated muscles are stretched by greater external load (e.g., bodyweight) that the force produced by the muscles, which are seen when sitting to a chair slowly, walking downhill or descending stairs, and resistance exercises such as lowering a dumbbell [22]. These eccentric exercises have garnered attention, since lengthening muscle contractions require less effort and are therefore metabolically less demanding, resulting in reduced fatigue [23]. Research has shown that oxygen and energy consumption are lower in eccentric cycling compared to conventional cycling performed at the same intensity [24]. Such aspects of eccentric exercises make them a good option for patients and frail individuals [25]. We provided this information to participants and asked them to rank their two exercises again in the second questionnaire to check if this information changes their exercise choices.
After choosing their exercises, participants performed a brief session of these exercises (chosen in the second questionnaire) under the supervision of the principal investigator (PI). Here, the participants were shown how to perform these exercises correctly and safely. The goal here was to distinguish between the theoretical and practical choices of exercises, whether the participants would be able to do these exercises correctly and safely, and if they would prefer to perform these exercises on a regular basis (Supplementary Materials 1, 2, jem.elmerpub.com).
Semi-structured interviews
We designed some questions for our interview based on existing behavioral research on exercise and nutrition. The interviews comprised a combination of semi-structured and open-ended questions to encourage participants to share their views in detail, allowing us to extract as much information as possible from the participants. Each interview lasted approximately 20 min, focusing on several key areas: 1) patient awareness and understanding of MASLD and its severity; 2) perceptions of exercise’s role in treatment of MASLD; 3) patient-reported barriers to and motivators of exercise; and 4) type of exercises that patients would choose to perform on a long-term basis and their reasons. The interviews were conducted in person by the PI. All interviews were audio recorded with the permission of the participant and were subsequently transcribed verbatim. The PI meticulously reviewed all the transcripts for accuracy by cross-referencing them with the audio recordings (Supplementary Materials 3, jem.elmerpub.com).
Statistical analyses
Quantitative statistical analyses were conducted using IBM SPSS Statistics for Windows, version 29.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics, using means, percentages, interquartile ranges, and standard deviations (SDs), were used to summarize the responses. Data are presented as mean ± SD of the mean. For qualitative analysis, the six steps of thematic analysis were followed [23]. The PI thoroughly reviewed all transcripts to become acquainted with the data. Initial codes were then generated for the data using NVIVO 12 Pro software (QRS International, Victoria, Australia). These codes were organized into categories to identify different themes and visualize the data. An inductive approach was adopted to ensure that the codes generated were solely derived from the collected data, reflecting the opinions expressed by the participants.
| Results | ▴Top |
Study population
A total of 21 participants, with a mean age of 59.1 ± 11.4 (range 37 - 76) years, and a mean body mass index (BMI) of 31.1 ± 4.8 (23 - 39), were enrolled in the study. Of these, 13 were female (62%) and eight were male participants. The CAP and liver stiffness measurement (LSM) scores were missing for six participants. The mean CAP score for the remaining 15 participants was 328.5 ± 44.6 (218 - 400), with an interquartile range of LSM scores of 3.6. Nine participants (43%) had type 2 diabetes mellitus (T2DM). Eighteen out of the 21 participants completed all three stages of the study. Interviews could not be conducted for three participants as they did not have the time to complete the session. No repeat or follow-up interviews were conducted in this study.
Emergent themes and codes
Table 2 outlines all the codes derived from the transcripts and the various categories of themes.
Click to view |
Table 2. List of Codes and the Categories of
Themes Generated From the Audio Transcripts |
Knowledge and perspectives about MASLD
Most participants (67%) exhibited some level of awareness regarding the cause and severity of MASLD. They were acquainted with the disease term as they had previously received a diagnosis of MASLD and were still experiencing symptoms at the time of the study. The most frequently voiced concern among participants was the potential adverse effects of disease progression on liver health.
Furthermore, certain participants expressed concerns regarding the detrimental effects of the disease on their overall health and well-being.
However, approximately one-third of the participants either lacked awareness or possessed limited knowledge about the disease. The primary reason cited for this lack of awareness was the scarcity of available information regarding the severity of the disease (Supplementary Material 4, jem.elmerpub.com).
Knowledge and perspectives about the role of exercise in MASLD treatment
While most participants recognized the awareness of MASLD and its severity, 56% were unaware of the role of exercise as part of the management strategy for MASLD. Some participants also expressed a lack of available information on this aspect, which would motivate them to seek further knowledge.
Although most participants lacked knowledge about the effectiveness of exercise in MASLD treatment, dietary modifications for managing MASLD appeared to be more widely recognized among them. Some participants mentioned their awareness of the importance of diet in managing the disease but were unaware of the role of exercise.
Interestingly, those who were aware of exercise’s potential role in MASLD management also believed that exercise should be complemented with dietary changes to experience the benefits in MASLD (Supplementary Material 4, jem.elmerpub.com).
Perspectives on the choice of exercises in questionnaires
Walking emerged as the top choice of exercise for 57% of the participants as their preferred long-term activity. More than 50% of participants highlighted the ease and portability of walking as their primary reasons, eloquently expressing their preference for this activity.
Additionally, a couple of participants emphasized the importance of enjoyment in exercise, noting that adherence to an exercise regimen is easier when the activity is enjoyable.
Resistance training with free weights and eccentric-biased bodyweight resistance exercise were selected as the second choice of exercises by 19% of the participants (Supplementary Material 4, jem.elmerpub.com).
Reasons for choosing resistance training with free weights
The primary reason cited for selecting resistance training with free weights was participants’ prior experience with this type of exercise, which proved to be one of the most influential factors.
Another significant factor in choosing this exercise was its convenience for home use, without the need for elaborate equipment, as succinctly expressed by several female participants.
Additionally, a couple of participants considered this type of exercise easy to perform due to its relatively low-impact nature (Supplementary Material 4, jem.elmerpub.com).
Reasons for choosing eccentric-biased bodyweight resistance exercise
Six participants identified the ease of performing eccentric-biased bodyweight resistance exercises as the primary reason for incorporating them into their daily routine if given a choice.
Not having access to a gym or simply not being enthusiastic about using fancy gym equipment was also a common factor influencing participants’ decision to opt for this type of exercise.
One participant also mentioned the portability of these exercises, emphasizing that they can be performed anywhere and at any time of the day (Supplementary Material 4, jem.elmerpub.com).
Perspectives on eccentric exercise
In the second questionnaire, 57% of the participants chose eccentric-biased exercise as one of their top two ranked exercises. Among them, half had altered their exercise preference to eccentric-biased exercise after receiving information provided to them in the presentation. Seven participants cited the less fatigue-inducing nature of eccentric exercise, coupled with its equal or greater benefits, as the primary reason for this change in perspective [24, 25]. Four participants were already aware of the benefits of eccentric contractions, which influenced their choice (Supplementary Material 4, jem.elmerpub.com).
Barriers to exercise
As noted previously, the majority of participants did not attribute a therapeutic status to exercise in the context of MASLD. Not having the time from their busy schedules to exercise regularly was the most commonly expressed barrier by the participants.
Lack of motivation to engage in regular exercise was also cited as one of the common barriers by participants.
Some people recognize the importance of regular exercise for maintaining their health and overall well-being. However, physical discomfort and fatigue induced by exercise also serve as significant barriers for some participants. For instance, a 69-year-old female had breathing difficulties, possibly linked to fatigue induced by fatty liver, which hinders her ability to exert herself during exercise and become hot and sweaty, conditions she believes are necessary to derive benefits from her exercise sessions.
Similarly, this person does not really enjoy exercising, possibly due to a perceived inability to perform the exercises correctly (Supplementary Material 4, jem.elmerpub.com).
Motivators to exercise
Although exercise was not widely favored among the majority of participants, they did express factors that could potentially motivate them to incorporate exercise into their lifestyle. Five participants mentioned a preference for exercises that would yield positive results for them. Four participants highlighted the importance of having correct knowledge about the role of exercise in managing the disease, the optimal exercise modality, and the correct technique for safe execution as key motivating factors.
Exercises that are quick and time-efficient were favored by a couple of participants. One participant emphasized that the importance of having support from family plays a critical role in encouraging you to adopt a healthy lifestyle with exercise (Supplementary Material 4, jem.elmerpub.com).
| Discussion | ▴Top |
To the best of our knowledge, this was the first qualitative study to assess the awareness, attitudes, behaviors, and exercise preferences of patients with MASLD. While a few qualitative studies have explored patient awareness and behaviors in relation to MASLD, none has specifically focused on exercise-related perspectives [17, 26]. Similar studies have been conducted for other chronic conditions, for instance, Peng et al [27] examined self-management behaviors in patients with type 2 diabetes and identified factors influencing those behaviors. However, these studies did not specifically aim to identify preferred types of exercises and reasons behind the preferences for exercise managing chronic metabolic diseases like MASLD that presents a significant challenge in healthcare, as these require long-term lifestyle behavioral changes. Despite extensive research on the efficacy of different types of structured exercises in MASLD treatment [7, 10], various factors such as disease symptoms, associated morbidity and mortality, or mental health issues influence individuals’ inclination to adopt these long-term behavioral changes. Therefore, identifying patient disease knowledge and their thoughts on exercise as a potential treatment option in MASLD via one-on-one interviews is necessary to develop individualized and sustainable exercise interventions tailored to personalized patient needs.
We found that the majority of participants were aware of MASLD and its potential consequences for liver health and also on overall well-being. Some participants attributed this awareness to information received from their healthcare providers, or their own research they did after receiving their diagnosis. This contrasts with findings from another qualitative study, in which ambiguity about the diagnosis and the cause of liver disease was prevalent [26]. Additionally, patients in the study also expressed dissatisfaction about the lack of information and explanations regarding their diagnosis [26]. This observation is consistent with our findings where one-third of our participants mentioned inadequate education from their doctor regarding the diagnosis and cause of fatty liver.
Regarding exercise as a treatment for MASLD, most participants were unaware of its significance. Importantly, they expressed dissatisfaction with the lack of available information and education from their doctors, including specific recommendations on how to leverage exercise as a treatment option. This aligns with the findings of previous studies where patients reported a lack of education and guidance from their treating provider on incorporating physical activity into routine care [12, 26]. Time constraints, lack of motivation, and physical discomfort and fatigue from exercise were common barriers to exercise cited by participants. These findings are consistent with recent questionnaire studies identifying fatigue and lack of time as common barriers to exercise in people with MASLD [13, 28]. Addressing low motivation to change exercise behaviors presents a significant challenge for both healthcare providers and patients themselves. Participants expressed a propensity towards exercises that were time-efficient and could give them the results that they desire. Other motivating factors included having correct knowledge on how and which type of exercise to implement, and the support available from family to implement these behavioral changes. These results emphasize the importance of individualized treatment approaches focused addressing these barriers and motivators to improve the uptake of exercise as a behavioral treatment option. However, participants demonstrated greater awareness about the role of dietary modifications compared to exercise. Although investigating participant perspectives on dietary implications was beyond the scope of our study, these findings suggest that diet certainly has garnered more attention among participants compared to exercise. Overall, raising awareness among these people by educating them on the importance of exercise in treating MASLD is crucial.
It is important for practitioners to know what kind of exercise patients would think that they could do regularly, and what are potential barriers for them to actually perform the exercise. It is also important for practitioners to provide patients with opportunities to try exercises of their choices to see how they feel when they perform the exercises. The present study found that walking was the most favorable exercise among participants (Fig. 1). Reasons for this choice included its easiness, flexibility, and enjoyment. Studies have shown that people with MASLD experience higher fatigue levels as they have poor cardiorespiratory fitness levels and a greater rate of perceived exertion during exercise, significantly impacting their ability and willingness to exercise regularly [15, 29]. This likely explains the reason why these people choose walking as their top preference pertaining to its low-exertion nature. The portability aspect of walking helps participants overcome time constraints, facilitating regular engagement in exercise. Participants also emphasized the importance of enjoyment to achieve long-term adherence to exercise.
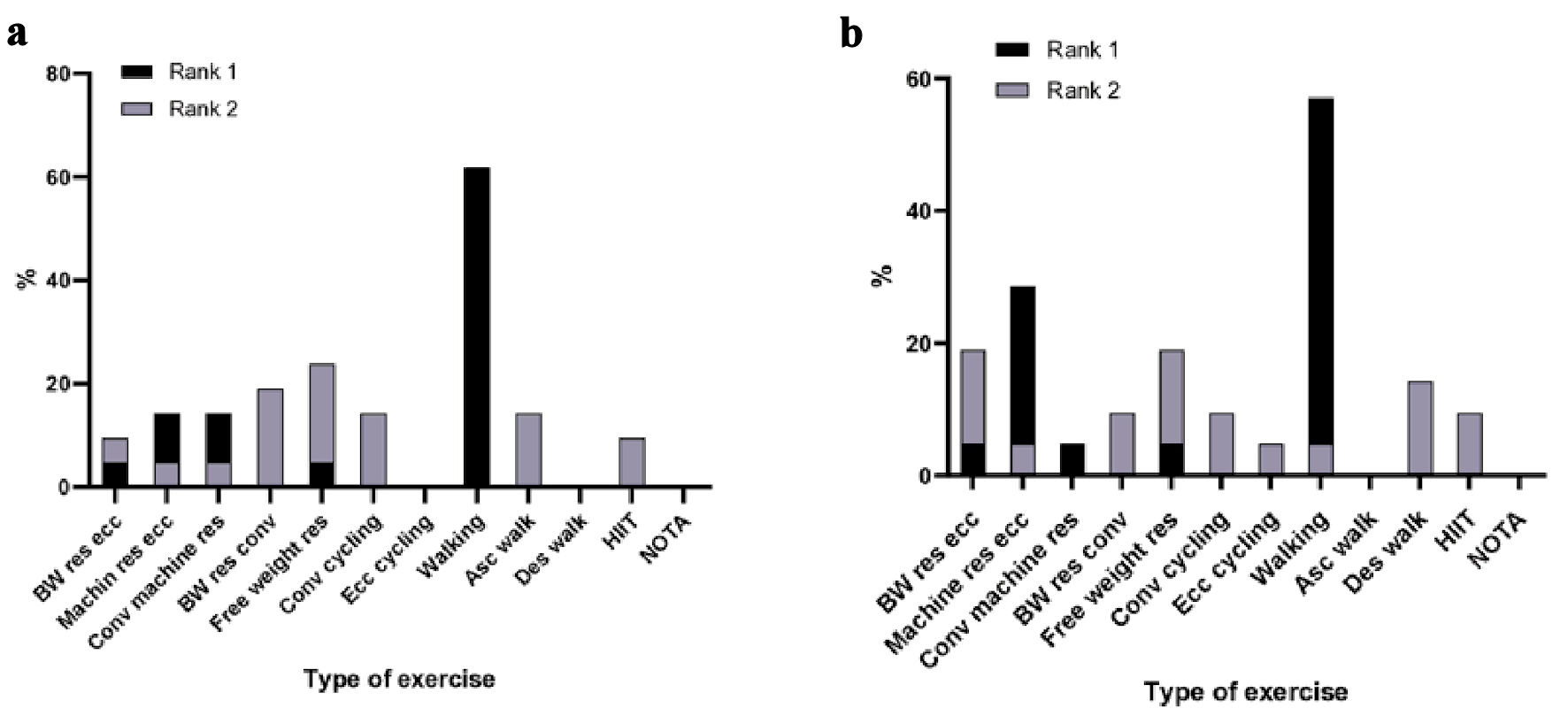 Click for large image |
Figure 1. Exercise choices of participants after watching the videos. (a) Ranking of top two exercises in questionnaire 1. (b) Ranking of top exercises in questionnaire 2. Walking was chosen by 57% as rank 1, and eccentric-biased bodyweight resistance and resistance exercise with free weights was chosen by 19% as rank 2. BW res ecc: body-weight resistance eccentric; Machin res ecc: machine resistance eccentric; Conv machine res: conventional machine resistance; BW res conv: body-weight resistance conventional; Free weight res: free weight resistance; Conv cycling: conventional cycling; Ecc cycling: eccentric cycling; Asc walk: ascending stair walking; Des walk: descending stair walking; HIIT: high-intensity interval training; NOTA: none of the above. |
Resistance training with free weights, such as dumbbells or any other form of weighted object, was one of the second most favored exercises (Fig. 1). Factors influencing this choice included prior experience, convenience for home use without any elaborate gym equipment, and its relatively low-impact nature. Bodyweight resistance exercise with a focus on eccentric contractions was also favored as the second choice of exercise. The major reasons driving this selection were the ease involved in performing these exercises, no requirement of having a gym membership and using the gym machines, and the portability of these exercises as they can be done anywhere with minimal to no equipment other than your bodyweight. Specifically, participants chose eccentric version of the bodyweight resistance exercise after learning about its less fatigue-inducing nature along with the potential of providing equal or greater benefits in some aspects. These findings suggest that people with MASLD prefer exercises that are easy to perform, not very strenuous, non-complex, and do not require gym attendance, and are easy to implement. This also corroborates with the concerns of fatigue caused by exercise and time constraints previously reported by people with MASLD [28]. This underscores the importance of personalized treatment approaches integrating exercise preferences and fitness levels of patients to maximize long-term adherence to exercise. The efficacy of eccentric exercise, particularly in MASLD, remains unexplored, offering a promising avenue for future research on this topic.
Several limitations in the present study should be addressed. The small sample size limited the breadth of perspectives obtained. Moreover, a majority of participants (76%) were Caucasians, potentially impacting the knowledge levels on disease, role of exercise, barriers and motivators to exercise, and also the exercise preferences. Overall, this could affect the generalizability and validity of the findings. Furthermore, exercise options provided did not include water-based exercises or yoga, which are gaining significant recognition and utility. Including these options may have impacted exercise choices. Although Fibroscan is a reliable tool for detecting liver fibrosis, accurately assessing liver steatosis (the fat content in the liver), particularly in obese participants, may pose challenges and potentially impact the results. Nevertheless, there are several strengths of this study. This study addresses a critical gap in literature by focusing on patient awareness and, more importantly, their preferences regarding exercise, providing valuable insights that are directly applicable to clinical practice. The use of both quantitative (questionnaire) and qualitative (personal interviews) methods provides a robust and comprehensive approach to understanding patient perspectives. This type of study design allows for a deeper exploration of the issues, combining statistical data with personal insights. Additionally, we selected the age range of ≥ 37 years based on the demographic most commonly seen in the outpatient hepatology setting during the recruitment period. Our goal was to focus on individuals most commonly diagnosed with MASLD in clinical settings. Future studies should consider including younger populations to improve generalizability. We also acknowledge that including an open-ended question in the final item of the questionnaire could have captured additional preferences for physical activity; this will be considered in future research. Although the interviews and assessments were conducted in person, participants were asked to report their most recent weight due to practical constraints during the interview process. However, all patients attending the FSH Hepatology Clinic routinely have their weight measured during appointments unless they are wheelchair-bound, and none of the participants in this study were wheelchair users. We acknowledge that using self-reported weight instead of directly accessing measured data may introduce reporting bias and have noted this as a methodological limitation.
In conclusion, this qualitative analysis provides valuable insights into the perspectives of people with MASLD regarding the disease, the role of exercise, the potential of exercise as a treatment option, and more importantly what type of exercises and behaviors would motivate them to embrace long-term behavioral changes. These findings underscore the urgent need for concise and informative educational material as part of standard of care to people with MASLD on the significance of exercise and how they can implement exercise to facilitate behavioral change. The findings of this study can guide future exercise intervention trials to investigate simple exercises based on preferences, improving long-term adherence. The information from such qualitative research studies can also be used to develop personalized health optimization and self-management packages, which can improve the uptake of behavioral changes, reducing the burden on healthcare system and improving clinical outcomes. Combining these strategies can deliver tailored care for people with MASLD, enhancing individualized patient care and leading to better clinical outcomes.
| Supplementary Material | ▴Top |
Suppl 1. Questionnaire 1.
Suppl 2. Questionnaire 2.
Suppl 3. Interview guide.
Suppl 4. Participants’ comments.
Acknowledgments
The authors thank all the study participants, as well as hepatology nurses Wendy Lam, Crystal Connelly, Marcelle Scagliotta, and Huirong Ma for their assistance with the project. We also thank Prof. George Garas and Dr. Raj Uchila for their assistance with patient recruitment.
Financial Disclosure
This work was supported by a PhD scholarship from Edith Cowan University. The university did not have any role in the study design, data collection, analysis or interpretation of the data; in writing this manuscript, or in the decision to submit the article for publication.
Conflict of Interest
The authors declare no conflict of interest that pertains to this work.
Informed Consent
Written informed consent was obtained prior to participation.
Author Contributions
Substantial contributions to study concepts and design: KD, OA, KN, JO. Acquisition of data: KD and OA. Analysis and interpretation of data: KD. Drafting of the manuscript: KD. Statistical analysis: KD. Figures and tables: KD, OA and KN. Critical revision of the manuscript for important intellectual content: KD, OA, KN and JO.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The
global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis
(NASH): a systematic review. Hepatology. 2023;77(4):1335-1347.
doi pubmed - Devarbhavi H, Asrani SK, Arab JP, Nartey YA, Pose E, Kamath PS.
Global burden of liver disease: 2023 update. J Hepatol. 2023;79(2):516-537.
doi pubmed - Fernando DH, Forbes JM, Angus PW, Herath CB. Development and
progression of non-alcoholic fatty liver disease: the role of advanced glycation end products.
Int J Mol Sci. 2019;20(20):5037.
doi pubmed - Adams LA, Roberts SK, Strasser SI, Mahady SE, Powell E, Estes C,
Razavi H, et al. Nonalcoholic fatty liver disease burden: Australia, 2019-2030.
J Gastroenterol Hepatol. 2020;35(9):1628-1635.
doi pubmed - Vaz K, Kemp W, Majeed A, Lubel J, Magliano DJ, Glenister KM, Bourke
L, et al. Non-alcoholic fatty liver disease prevalence in Australia has risen over 15 years in
conjunction with increased prevalence of obesity and reduction in healthy lifestyle.
J Gastroenterol Hepatol. 2023;38(10):1823-1831.
doi pubmed - Younossi ZM, Zelber-Sagi S, Henry L, Gerber LH. Lifestyle
interventions in nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol.
2023;20(11):708-722.
doi pubmed - Heinle JW, DiJoseph K, Sabag A, Oh S, Kimball SR, Keating S, Stine
JG. Exercise is medicine for nonalcoholic fatty liver disease: exploration of putative
mechanisms. Nutrients. 2023;15(11):2452.
doi pubmed - Stine JG, Long MT, Corey KE, Sallis RE, Allen AM, Armstrong MJ,
Conroy DE, et al. American College of Sports Medicine (ACSM) International Multidisciplinary
Roundtable report on physical activity and nonalcoholic fatty liver disease. Hepatol Commun.
2023;7(4):e0108.
doi pubmed - European Association for the Study of the Liver, European Association
for the Study of Diabetes, European Association for the Study of Obesity. EASL-EASD-EASO
Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease.
J Hepatol. 2016;64(6):1388-1402.
doi pubmed - Hashida R, Kawaguchi T, Bekki M, Omoto M, Matsuse H, Nago T, Takano
Y, et al. Aerobic vs. resistance exercise in non-alcoholic fatty liver disease: A systematic
review. J Hepatol. 2017;66(1):142-152.
doi pubmed - Hallsworth K, Adams LA. Lifestyle modification in NAFLD/NASH: Facts
and figures. JHEP Rep. 2019;1(6):468-479.
doi pubmed - Stine JG, Soriano C, Schreibman I, Rivas G, Hummer B, Yoo E, Schmitz
K, et al. Breaking down barriers to physical activity in patients with nonalcoholic fatty liver
disease. Dig Dis Sci. 2021;66(10):3604-3611.
doi pubmed - Glass O, Liu D, Bechard E, Guy CD, Pendergast J, Mae Diehl A,
Abdelmalek MF. Perceptions of exercise and its challenges in patients with nonalcoholic fatty
liver disease: a survey-based study. Hepatol Commun. 2022;6(2):334-344.
doi pubmed - Golabi P, Otgonsuren M, Cable R, Felix S, Koenig A, Sayiner M,
Younossi ZM. Non-alcoholic Fatty Liver Disease (NAFLD) is associated with impairment of Health
Related Quality of Life (HRQOL). Health Qual Life Outcomes. 2016;14:18.
doi pubmed - Mitchell T, McKinnon E, Ayonrinde O, Adams LA, Trinder D, Chua ACG,
Newton RU, et al. Decreased physical working capacity in adolescents with nonalcoholic fatty
liver disease associates with reduced iron availability. Clin Gastroenterol Hepatol.
2020;18(7):1584-1591.
doi pubmed - Prasun P, Ginevic I, Oishi K. Mitochondrial dysfunction in
nonalcoholic fatty liver disease and alcohol related liver disease. Transl Gastroenterol
Hepatol. 2021;6:4.
doi pubmed - Alemany-Pages M, Moura-Ramos M, Araujo S, Macedo MP, Ribeiro RT, do
OD, Ramalho-Santos J, et al. Insights from qualitative research on NAFLD awareness with a cohort
of T2DM patients: time to go public with insulin resistance? BMC Public Health.
2020;20(1):1142.
doi pubmed - Avery L, Exley C, McPherson S, Trenell MI, Anstee QM, Hallsworth K.
Lifestyle behavior change in patients with nonalcoholic fatty liver disease: a qualitative study
of clinical practice. Clin Gastroenterol Hepatol. 2017;15(12):1968-1971.
doi pubmed - Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F,
Romero D, et al. A multisociety Delphi consensus statement on new fatty liver disease
nomenclature. J Hepatol. 2023;79(6):1542-1556.
doi pubmed - Oh S, So R, Shida T, Matsuo T, Kim B, Akiyama K, Isobe T, et al.
High-intensity aerobic exercise improves both hepatic fat content and stiffness in sedentary
obese men with nonalcoholic fatty liver disease. Sci Rep. 2017;7:43029.
doi pubmed - Takahashi A, Abe K, Usami K, Imaizumi H, Hayashi M, Okai K, Kanno Y,
et al. Simple resistance exercise helps patients with non-alcoholic fatty liver disease.
Int J Sports Med. 2015;36(10):848-852.
doi pubmed - Douglas J, Pearson S, Ross A, McGuigan M. Chronic adaptations to
eccentric training: a systematic review. Sports Med. 2017;47(5):917-941.
doi pubmed - Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006;3(2):77-101.
- Chen TC, Hsieh CC, Tseng KW, Ho CC, Nosaka K. Effects of descending
stair walking on health and fitness of elderly obese women. Med Sci Sports Exerc.
2017;49(8):1614-1622.
doi pubmed - Julian V, Thivel D, Costes F, Touron J, Boirie Y, Pereira B, Perrault
H, et al. Eccentric training improves body composition by inducing mechanical and metabolic
adaptations: a promising approach for overweight and obese individuals. Front Physiol.
2018;9:1013.
doi pubmed - Tincopa MA, Wong J, Fetters M, Lok AS. Patient disease knowledge,
attitudes and behaviours related to non-alcoholic fatty liver disease: a qualitative study. BMJ
Open Gastroenterol. 2021;8(1):e000634.
doi pubmed - Peng X, Guo X, Li H, Wang D, Liu C, Du Y. A qualitative exploration
of self-management behaviors and influencing factors in patients with type 2 diabetes. Front
Endocrinol (Lausanne). 2022;13:771293.
doi pubmed - Deshpande K, Olynyk J, Ayonrinde O, Nosaka K. Barriers to exercise in
patients with metabolic dysfunction-associated steatotic liver disease: a patient survey.
J Clin Med Res. 2024;16(2-3):94-105.
doi pubmed - Weinstein AA, Escheik C, Oe B, Price JK, Gerber LH, Younossi ZM.
Perception of effort during activity in patients with chronic hepatitis c and nonalcoholic fatty
liver disease. PM R. 2016;8(1):28-34.
doi pubmed
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Endocrinology and Metabolism is published by Elmer Press Inc.