| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Case Report
Volume 16, Number 1, February 2026, pages 38-43

Disappearing Thyroid Nodules: A Case Report and Review of Evidence
Tonet Seres-Noriegaa, c, Antonio J. Amorb
aEndocrinology and Nutrition, Centro Medico Milenium, Zaragoza,
Spain
bDiabetes Unit, Endocrinology and Nutrition Department, Hospital Clinic,
Barcelona, Spain
cCorresponding Author: Tonet Seres-Noriega, Endocrinology and
Nutrition, Centro Medico Milenium, 50006 Zaragoza, Spain
Manuscript submitted October 3, 2025, accepted December 22, 2025, published online January 4,
2026
Short title: Disappearing Thyroid Nodules
doi: https://doi.org/10.14740/jem1575
| Abstract | ▴Top |
We present the case of a 24-year-old African-American woman who noticed an anterior cervical mass during self-examination 2 weeks prior. Although she experienced no compressive, local or systemic symptoms, she expressed aesthetic concerns. Ultrasound findings identified a single left thyroid nodule, cystic and with internal septations and eccentric solid areas (EU-TIRADS 2) measuring 22.9 mm in maximum diameter, warranting fine-needle aspiration (FNA) due to aesthetic concerns. Initial blood tests showed no inflammatory markers or thyroid axis abnormalities. Despite recommendations for therapeutic intervention, the patient declined the procedure after observing a reduction in the mass. Four months later, follow-up ultrasound revealed complete resorption of the nodule. This report reviews evidence on thyroid nodule disappearance/resorption, emphasizing the importance of individualized, patient-centered care.
Keywords: Thyroid nodule; Thyroid cyst; Spontaneous resolution; Resorption; Disappearance; Thyroid ultrasound
| Introduction | ▴Top |
This case report presents a remarkable instance of complete spontaneous resolution of a cystic thyroid nodule in a young woman, representing an uncommon phenomenon within the natural history of thyroid nodules. According to a recent systematic review and meta-analysis, thyroid nodules have a prevalence of approximately 25% in the general population, particularly among women [1]. While most are discovered incidentally and are small in size and clinically insignificant, up to 10-15% may be malignant [2]. The natural history of thyroid nodules varies widely, with limited data available on shrinking or disappearing nodules.
A multicenter, prospective European study involving 992 patients indicated that over 5 years of follow-up, benign thyroid nodules tend to grow in approximately 15% of cases, remain stable in approximately 70% of cases, and shrink in another 15% of cases [3]. Among the factors that have been associated with growth are the presence of multiple nodules, larger nodule size, male sex, and young age [3]. However, the natural history of thyroid nodules rarely ends in their complete resolution [4].
This case is particularly noteworthy as it involves complete resolution of a large cystic nodule that exceeded 20 mm in diameter, a phenomenon that challenges conventional management approaches and highlights the importance of individualized patient care.
| Case Report | ▴Top |
Investigations
A 24-year-old African-American woman presented to the endocrinology clinic with a left anterior cervical mass that she detected during self-examination 2 weeks earlier. The mass was painless and caused no compressive symptoms at the tracheoesophageal or neurological levels, though it represented a significant cosmetic concern for the patient. There were no accompanying signs or symptoms of cervical or systemic inflammation.
The patient reported no known drug allergies and admitted to occasional smoking and alcohol consumption. She had no history of thyroid disease but reported a maternal history of primary hypothyroidism. No family history of nodular or malignant thyroid pathology was noted.
The patient had a history of grade III obesity (maximum weight: 132 kg, height: 170 cm, body mass index (BMI): 45.7 kg/m2). With improved lifestyle habits, including daily physical activity and nutritional counseling, she achieved a weight loss of 42.6 kg over 2 - 3 years (current weight: 89.4 kg, BMI: 30.9 kg/m2).
Additionally, she had undergone tonsillectomy for recurrent tonsillitis. Her regular medications included combined oral hormonal contraception (ethinylestradiol 30 µg and levonorgestrel 150 µg, Seasonique®). There was no history of radiation exposure to the head and neck region.
Clinical findings
Physical examination revealed several important findings that guided subsequent management decisions. The examination identified a small, mobile, non-painful, soft, compressible mass located in the left anterior neck region. The mass demonstrated mobility with swallowing and the patient exhibited no signs of compressive symptomatology. Importantly, there was no evidence of lateral neck lymphadenopathy, which would have raised suspicion for malignant disease. The examination also revealed no signs of thyroid ophthalmopathy, and the remainder of the thyroid gland appeared normal on palpation.
Diagnostic assessment
Initial blood tests confirmed euthyroidism (thyroid-stimulating hormone (TSH): 3.51 µU/mL (0.35 - 4.94); free T4: 0.97 ng/dL (0.7 - 1.48)), and inflammatory markers were within normal ranges. Other serum biochemical parameters showed no significant abnormalities.
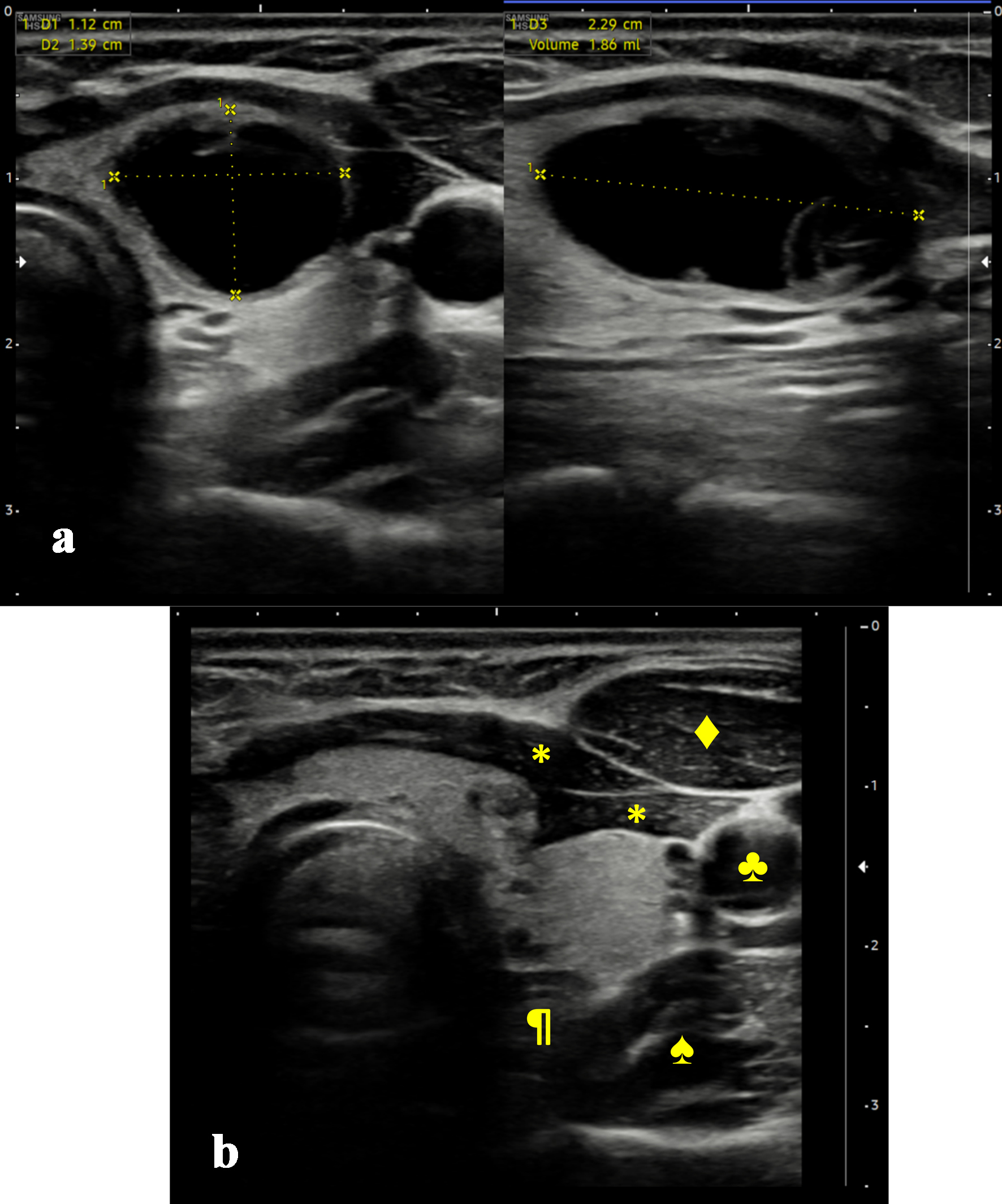
Cervical ultrasound (Fig. 1a) showed a normal-sized thyroid gland with homogeneous parenchyma and no increased Doppler signal. A solitary left lower thyroid nodule with regular shape, well-defined margins, cystic content, and internal septations was observed. It measured 11.2 × 13.9 × 22.9 mm (anteroposterior × transverse × longitudinal axes) and had a volume of 1.86 cc. Posterior peripheral areas showed minimal isoechoic, homogeneous content. The absence of vascularity and microcalcifications in these regions is compatible with intracystic debris. There was no central or lateral neck adenopathy suggestive of malignancy.
 Click for large image |
Figure 1. Initial and follow-up thyroid ultrasound images. (a) Initial ultrasound images (anteroposterior and longitudinal axes, respectively). (b) Follow-up ultrasound image after 4 months (anteroposterior axis). *: strap muscles; ♣: left common carotid artery; ♦: left sternocleidomastoid muscle; ♠: left Longus colli muscle; ¶: esophagus. |
Therapeutic intervention
According to European Thyroid Imaging Reporting and Data System (EU-TIRADS) classification, the nodule was categorized as EU-TIRADS 2, and fine-needle aspiration (FNA) was recommended for therapeutic purposes [5]. The recommended approach for such predominantly cystic nodules, which cause aesthetic concerns, involves draining the cystic content. Despite the high recurrence rate of thyroid cysts, simple drainage offers satisfactory results in up to approximately 20% of cases [4]. In case of symptomatic recurrence, ethanol ablation, preferably, or surgery can be performed [6, 7].
The guidelines of the American Thyroid Association (ATA) [6] recommend performing FNA in nodules with suspicious ultrasound features based on their size. In the reported case, it would be classified as benign and FNA is recommended only as therapeutic intervention. According to the European Thyroid Association (ETA) guidelines [7], the recommended approach is to proceed as described above: FNA for EU-TIRADS 2 for therapeutic purposes.
Follow-up and outcomes
Four months later, the patient reported gradual shrinkage of the cervical mass, which had become asymptomatic. Follow-up ultrasound demonstrated complete resorption of the nodule. Anterior capsular and infrahyoid muscle retraction (notably the left sternothyroid muscle) was noted (Fig. 1b). Given the patient’s asymptomatic status, periodic ultrasound follow-up was agreed upon. The timeline of this case is shown in Table 1.
 Click to view |
Table 1. Chronology of Events and Clinical
Evolution |
From a patient-assessed outcome perspective, the resolution of cosmetic concerns represented the primary treatment goal, which was achieved without invasive intervention. The patient expressed satisfaction with the conservative approach and relief regarding the benign course of the nodule.
The tolerability of the watchful waiting approach was optimal, as it involved no procedural discomfort or complications associated with invasive diagnostics. No adverse or unanticipated events occurred during the observation period. The complete resolution eliminated concerns about potential complications from FNA, such as bleeding, infection, or technical difficulties. The outcome also avoided potential psychological distress associated with an inadequate or indeterminate cytology result, which occurs in a significant percentage of thyroid FNA specimens.
| Discussion | ▴Top |
This case demonstrates several important clinical lessons regarding the natural history of thyroid nodules and the value of individualized patient management. The complete spontaneous resolution of a large, predominantly cystic thyroid nodule represents an uncommon phenomenon that challenges rigid adherence to clinical management protocols.
Initial evaluation includes clinical history and physical examination to narrow differential diagnoses. For masses of thyroid origin, key aspects include appearance, characteristics, associated symptoms, risk factors (e.g., prior cervical radiation), and family history of thyroid malignancy. Additionally, functionalism, mainly hyperthyroidism or thyrotoxicosis, should be ruled out by anamnesis of suggestive symptoms, determination of serum TSH and, if below normal, an assessment of the use of radionuclide thyroid scan (preferably I123).
The imaging test of choice to assess thyroid tissue is cervical ultrasound using a high-frequency linear probe (e.g., up to 14 MHz). No single feature assessed by ultrasound offers sufficient diagnostic yield to dictate, by itself, the likelihood of malignancy of a thyroid nodule. For this reason, multiple classification systems guide the indication for FNA based on a set of specific features, including the EU-TIRADS [5], the American College of Radiology TIRADS (ACR-TIRADS) [8], Korean TIRADS (K-TIRADS) [9], and ATA 2015 guidelines [6]. Although efforts are being made to develop an International TIRADS (I-TIRADS) [10], European guidelines recommend the use of the EU-TIRADS classification [5, 7]. In the case reported, the nodule was classified as EU-TIRADS 2 and FNA was recommended due to aesthetic concerns.
Thyroid nodules’ natural history varies widely, with limited data on shrinking or disappearing nodules. The frequency of thyroid nodule reduction, using different definition criteria, has been estimated at 13.1-33.1% (Table 2) [3, 4, 11-19]. Spontaneous resolution ranges from 2.5% to 34% (Table 2). It is noteworthy that in many of the studies, prior FNA had been performed, which may alter the natural course of the nodule by draining or obliterating it [20]. A Korean study, particularly relevant to the reported case because of its similarity, followed 59 subjects with predominantly cystic nodules > 20 mm in maximum diameter for one and a half years without performing FNA [4]. The study observed partial collapse in 22% of cases, with no instances of total collapse, emphasizing the unusual nature of the current case [4].
Click to view |
Table 2. Summary of the Characteristics of
Studies Reporting Frequencies of Thyroid Nodule Reduction and Disappearance
(Reverse Chronological Order) |
Additionally, a population-based study in Denmark involving 2,465 adults showed approximately 24% disappearance of nodules after an iodization program and 11 years of follow-up [11]. Living in the most iodine-deficient region prior to the program was the sole parameter associated with nodule disappearance in multivariate models [11]. Other potential predictors of nodular disappearance include cystic and small-size content [12] or nodules/pseudo-nodules in the context of thyroiditis [21]. The main studies that have reported frequencies of thyroid nodule shrinkage and/or disappearance are summarized in Table 2.
Current clinical practice guidelines do not specifically address the management of patients who decline recommended FNA, creating uncertainty about optimal surveillance strategies. Once benignity has been confirmed, various therapeutic options can be considered for large, compressive nodules or those causing aesthetic concerns. The ATA recommends surgical excision or ethanol ablation for recurrent cystic nodules [6]. The ETA designates ethanol ablation as the preferred method for such nodules, with thermal ablation as a secondary option in cases where ethanol ablation fails [7].
From a broader clinical perspective, this case highlights the importance of patient-centered care and individualized treatment decisions. While guidelines provide important frameworks for clinical decision-making, they cannot account for all clinical scenarios or patient preferences. The successful outcome in this case demonstrates that careful observation with appropriate surveillance can be a viable management strategy in selected patients with cystic thyroid nodules.
The primary take-away lessons from this case report encompass several important clinical principles. Spontaneous resolution of thyroid nodules, while uncommon, represents an important aspect of their natural history that clinicians should discuss with patients during counseling about management options. The phenomenon of complete nodule resolution, particularly in large cystic lesions, suggests that the natural history of thyroid nodules is more variable than previously understood, and that adherence to size-based FNA criteria may not always be necessary. Individualized management approaches that incorporate patient preferences alongside clinical guidelines can lead to favorable outcomes when combined with appropriate surveillance and patient education. The case demonstrates that shared decision-making should be respected when clinical circumstances allow, while maintaining appropriate safety measures through regular monitoring. Patients should be informed about the potential for natural resolution, especially in cases involving cystic nodules, while maintaining appropriate surveillance to ensure patient safety. Finally, this case contributes to the growing body of literature suggesting that watchful waiting may be appropriate for selected thyroid nodules, particularly those with benign imaging characteristics in compliant patients who understand the importance of regular follow-up.
Acknowledgments
The authors would like to thank the patient for her cooperation throughout the study.
Financial Disclosure
No financial support or funding was received for the preparation of this manuscript.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Informed consent was obtained from the patient.
Author Contributions
TSN carried out the clinical assessment, ultrasound examination, follow-up, and drafted the manuscript. Both TSN and AJA reviewed the relevant literature. AJA provided a critical review of the manuscript. Both authors reviewed the results and approved the final version of the manuscript.
Data Availability
The data that support the findings of this study are available from the authors upon reasonable request.
| References | ▴Top |
- Mu C, Ming X, Tian Y, Liu Y, Yao M, Ni Y, Liu Y, et al. Mapping
global epidemiology of thyroid nodules among general population: A systematic review and
meta-analysis. Front Oncol. 2022;12:1029926.
doi pubmed - Alexander EK, Cibas ES. Diagnosis of thyroid nodules. Lancet Diabetes
Endocrinol. 2022;10(7):533-539.
doi pubmed - Durante C, Costante G, Lucisano G, Bruno R, Meringolo D, Paciaroni A,
Puxeddu E, et al. The natural history of benign thyroid nodules. JAMA.
2015;313(9):926-935.
doi pubmed - Choi WJ, Baek JH, Choi YJ, Lee JH, Ha EJ, Lee WC, Lim HK, et al.
Management of cystic or predominantly cystic thyroid nodules: role of simple aspiration of
internal fluid. Endocr Res. 2015;40(4):215-219.
doi pubmed - Russ G, Bonnema SJ, Erdogan MF, Durante C, Ngu R, Leenhardt L.
European Thyroid Association Guidelines for ultrasound malignancy risk stratification of thyroid
nodules in adults: the EU-TIRADS. Eur Thyroid J. 2017;6(5):225-237.
doi pubmed - Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov
YE, Pacini F, et al. 2015 American Thyroid Association Management Guidelines for adult patients
with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association
Guidelines Task Force on thyroid nodules and differentiated thyroid cancer. Thyroid.
2016;26(1):1-133.
doi pubmed - Durante C, Hegedus L, Czarniecka A, Paschke R, Russ G, Schmitt F,
Soares P, et al. 2023 European Thyroid Association Clinical Practice Guidelines for thyroid
nodule management. Eur Thyroid J. 2023;12(5).
doi pubmed - Tessler FN, Middleton WD, Grant EG, Hoang JK, Berland LL, Teefey SA,
Cronan JJ, et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the
ACR TI-RADS Committee. J Am Coll Radiol. 2017;14(5):587-595.
doi pubmed - Ha EJ, Chung SR, Na DG, Ahn HS, Chung J, Lee JY, Park JS, et al. 2021
Korean thyroid imaging reporting and data system and imaging-based management of thyroid
nodules: Korean society of thyroid radiology consensus statement and recommendations.
Korean J Radiol. 2021;22(12):2094-2123.
doi pubmed - Durante C, Hegedus L, Na DG, Papini E, Sipos JA, Baek JH, Frasoldati
A, et al. International Expert Consensus on US Lexicon for Thyroid Nodules. Radiology.
2023;309(1):e231481.
doi pubmed - Krejbjerg A, Bjergved L, Pedersen IB, Knudsen N, Jorgensen T, Perrild
H, Ovesen L, et al. Thyroid nodules in an 11-year DanThyr follow-up study. J Clin
Endocrinol Metab. 2014;99(12):4749-4757.
doi pubmed - Rago T, Chiovato L, Aghini-Lombardi F, Grasso L, Pinchera A, Vitti P.
Non-palpable thyroid nodules in a borderline iodine-sufficient area: detection by
ultrasonography and follow-up. J Endocrinol Invest. 2001;24(10):770-776.
doi pubmed - Bajuk Studen K, Gaberscek S, Pirnat E, Zaletel K. Five-year follow-up
and clinical outcome in euthyroid patients with thyroid nodules. Radiol Oncol.
2021;55(3):317-322.
doi pubmed - Mohammadi M, Betel C, Burton KR, Higgins KM, Ghorab Z, Halperin IJ.
Follow-up of benign thyroid nodules-can we do less? Can Assoc Radiol J.
2019;70(1):62-67.
doi pubmed - Bhatia P, Deniwar A, Mohamed HE, Sholl A, Murad F, Aslam R, Kandil E.
Vanishing tumors of thyroid: histological variations after fine needle aspiration. Gland Surg.
2016;5(3):270-277.
doi pubmed - Erdogan MF, Gursoy A, Erdogan G. Natural course of benign thyroid
nodules in a moderately iodine-deficient area. Clin Endocrinol (Oxf).
2006;65(6):767-771.
doi pubmed - Brander AE, Viikinkoski VP, Nickels JI, Kivisaari LM. Importance of
thyroid abnormalities detected at US screening: a 5-year follow-up. Radiology.
2000;215(3):801-806.
doi pubmed - Kuma K, Matsuzuka F, Yokozawa T, Miyauchi A, Sugawara M. Fate of
untreated benign thyroid nodules: results of long-term follow-up. World J Surg.
1994;18(4):495-498; discussion 499.
doi pubmed - Ng EH, Tan SK, Nambiar R. Impact of fine needle aspiration cytology
on the management of solitary thyroid nodules. Aust N Z J Surg.
1990;60(6):463-466.
doi pubmed - Eze OP, Cai G, Baloch ZW, Khan A, Virk R, Hammers LW, Udelsman R, et
al. Vanishing thyroid tumors: a diagnostic dilemma after ultrasonography-guided fine-needle
aspiration. Thyroid. 2013;23(2):194-200.
doi pubmed - Kok CYZ, Liew H, Khoo HW, Li H. Thyroid nodules that disappear-a case report on pseudonodules in thyroiditis. Ann Thyroid. 2024;9(0).
This
article is distributed under the terms of the Creative Commons Attribution 4.0 International
License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any
medium, including commercial use, provided the original work is properly
cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.