| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Original Article
Volume 15, Number 5, December 2025, pages 210-219

Diabetes Drives Cardiovascular Risk in the Metabolic Triad: An Eight-Year Occupational Cohort Study of Ten Thousand Workers
Lupita Ana Maria Valladolid-Sandovala, Jhosmer Ballena-Caicedoa, Fiorella E. Zuzunaga-Montoyab, Victor Juan Vera-Poncea, c
aFacultad de Medicina (FAMED), Universidad Nacional Toribio Rodriguez de Mendoza de
Amazonas (UNTRM), Amazonas, Peru
bUniversidad Continental, Lima,
Peru
cCorresponding Author: Victor Juan Vera-Ponce, Facultad de Medicina
(FAMED), Universidad Nacional Toribio Rodriguez de Mendoza de Amazonas (UNTRM), Amazonas, Peru
Manuscript submitted October 7, 2025, accepted November 29, 2025, published online December 24,
2025
Short title: Diabetes and CVD Risk in the Metabolic Triad
doi:
https://doi.org/10.14740/jem1583
| Abstract | ▴Top |
Background: Cardiovascular diseases remain the leading cause of death and maintain a high burden in Latin America. Obesity, hypertension, and type 2 diabetes are independent risk factors, but their coexistence could amplify cardiovascular damage beyond their individual sum. The aim of our study was to determine, in a Peruvian occupational cohort followed for 8 years, how the coexistence of obesity, hypertension, and diabetes is associated with the incidence of major cardiovascular events and to identify which combinations confer the highest risk.
Methods: This was a retrospective observational cohort study of Peruvian workers without cardiovascular history, followed for 8 years. Obesity, hypertension, and diabetes were evaluated in eight mutually exclusive categories. The outcome was cardiovascular disease. Adjusted risk ratios were estimated using Cox regression, adjusted for age, sex, cholesterol, and triglycerides.
Results: A progressive risk increase pattern was observed where the group without components had an incidence of 1.30 per 1,000 person-years, while the triad reached 34.94 per 1,000 person-years with adjusted hazard ratio (aHR) = 10.87 (2.81 - 42.06). Among isolated components, diabetes showed the highest risk (aHR = 4.24; 1.36 - 13.35) compared to obesity (1.45; 0.68 - 3.10) and hypertension (1.17; 0.32 - 4.24). In combinations, obesity + diabetes (aHR = 6.34; 1.73 - 23.27) and diabetes + hypertension (5.86; 1.47 - 23.39) concentrated the highest risks, above obesity + hypertension (2.01; 0.71 - 5.72).
Conclusions: In the working population, the coexistence of obesity, hypertension, and diabetes progressively increases CVD risk, with diabetes as the main axis and the triad identifying a very high-risk subgroup. These findings support periodic screening and intensive multifactorial management in the occupational setting, prioritizing those presenting diabetes alone or in combination.
Keywords: Obesity; Body mass index; Diabetes mellitus; Hypertension; Epidemiologic factors; Public health
| Introduction | ▴Top |
Cardiovascular disease (CVD) constitutes the leading cause of mortality worldwide, accounting for approximately 18.6 million annual deaths, representing 31% of all global deaths [1]. In Latin America and the Caribbean, this problem acquires critical dimensions, where CVD represents approximately 1 million annual deaths, with a regional age-standardized prevalence of 7.0% [2]. Despite a 69.8% decrease in age-standardized mortality rates since 1990, absolute numbers have increased by 71.2%, reflecting population aging and epidemiological transition [3]. The economic impact in the region is devastating, with an estimated cost of 31 billion dollars annually in nine Latin American countries [4].
Obesity, arterial hypertension, and type 2 diabetes mellitus are consistently recognized as independent risk factors for major cardiovascular events. Large-scale studies such as INTERHEART have demonstrated that these modifiable factors account for a substantial proportion of population-attributable risk for myocardial infarction globally [5]. Furthermore, metabolic syndrome confers a relative risk of approximately two-fold for cardiovascular disease [6]. Likewise, even with optimal control, type 2 diabetes is associated with an approximately 45% increase in heart failure risk [7]. In Latin America, hypertension represents the risk factor with the highest population attributable fraction for cardiovascular events (18.7%), followed by abdominal obesity (15.4%) and diabetes (5.3%) [8]. However, the simultaneous coexistence of these three metabolic conditions, termed the “metabolic triad,” could generate a synergistic effect that amplifies cardiovascular risk beyond the simple sum of their individual effects. Unlike metabolic syndrome, which functions as a dichotomous diagnostic label implicitly assuming equivalent contributions from all its components, the metabolic triad approach allows for the disaggregated evaluation of obesity, hypertension, and diabetes - both individually and in specific combinations - to determine whether each component carries equal weight or whether one acts as the primary driver of cardiovascular risk. Furthermore, these three conditions represent established clinical diagnoses per se, routinely assessed in occupational health evaluations, facilitating practical risk stratification.
Despite the epidemiological relevance of this phenomenon, significant research gaps remain. First, available evidence comes predominantly from studies in general populations or hospital settings, while active workers, a relatively young and healthy population with access to periodic medical evaluations, have received limited research attention. Second, this knowledge gap is particularly pronounced in Latin America, where longitudinal cohort studies are scarce, limiting the generalizability of findings from European or North American populations to different socioeconomic and genetic contexts. Third, cardiovascular risk models specific to Latin American populations have not been developed to date, hindering the design of culturally adapted preventive strategies for working populations [9].
In this context, the present study analyzes an 8-year follow-up cohort of workers evaluated at an occupational clinic in Peru. The primary objective was to estimate the incidence of major cardiovascular events and evaluate the association between different combinations of the metabolic triad components (obesity, hypertension, and diabetes) and cardiovascular risk, using hazard ratios (HRs) derived from Cox regression models. The secondary objective was to identify which specific metabolic combinations confer the highest cardiovascular risk and to determine whether any single component acts as the primary driver of risk within the triad. Identifying which metabolic combinations confer the highest risk could enable more efficient allocation of preventive resources in occupational settings, where periodic health evaluations offer a unique opportunity for early intervention.
| Materials and Methods | ▴Top |
Study type and design
This was a retrospective observational cohort study based on systematic clinical records of workers evaluated at an occupational clinic in Peru. Data were originally collected prospectively as part of routine occupational medical surveillance over an 8-year period (2014 - 2021), during which clinical, anthropometric, and laboratory information was gathered, along with identification of major cardiovascular events. However, the present analysis was conducted retrospectively using these pre-existing records, which were not originally collected for research purposes.
Population, sample, and eligibility criteria
The cohort comprised working adults of both sexes, aged between 18 and 65 years, from different occupational settings. All participants were evaluated through a standardized occupational medical surveillance program, implemented in three specific stages of their work trajectory: pre-occupational evaluation (at entry), periodic evaluations (during work performance), and post-occupational evaluation (at termination of employment).
Inclusion criteria included participants who were working at study initiation and had complete records of blood pressure, glucose levels, and anthropometric parameters (such as weight and height), as well as their covariates. Additionally, completion of at least two clinical evaluations separated by a minimum interval of 1 year was required to allow follow-up of the metabolic triad components. Individuals with a history of cardiovascular disease (such as myocardial infarction or stroke) at baseline or with incomplete information on study variables were excluded.
As this study is based on secondary data originally collected for occupational surveillance purposes, a formal a priori sample size calculation was not applicable. A non-probabilistic consecutive sampling approach was employed, including all workers from the clinic’s database who met the eligibility criteria during the study period (2014 - 2021). Additionally, the completeness of clinical and laboratory data depended on the specific evaluations requested by each employer, as occupational surveillance protocols vary according to job risk profiles and company requirements. Workers whose employers did not request glucose measurement, blood pressure assessment, or anthropometric evaluation were not included due to missing exposure data.
Variables and measurement
The main exposure variables were arterial hypertension, obesity, and type 2 diabetes mellitus. Hypertension was defined as systolic blood pressure values ≥ 140 mm Hg or diastolic ≥ 90 mm Hg [10], or self-reported physician diagnosis of hypertension. Obesity was established using either a body mass index (BMI) > 30 kg/m2 or abdominal obesity defined as abdominal circumference (AC) ≥ 88 cm in women and ≥ 102 cm in men. Type 2 diabetes mellitus was determined by fasting plasma glucose levels ≥ 126 mg/dL after a minimum 8-h period without caloric intake [11], or self-reported physician diagnosis of diabetes. From these three conditions, a composite variable was constructed that classified participants into eight mutually exclusive categories: 1) no condition (reference group); 2) obesity only; 3) hypertension only; 4) diabetes only; 5) obesity and diabetes; 6) diabetes and hypertension; 7) obesity and hypertension; and 8) all three conditions simultaneously.
Primary outcomes were incident major cardiovascular events, defined as the first documented occurrence of acute myocardial infarction or stroke during the follow-up period. Event ascertainment followed a two-stage process: initial identification occurred during periodic occupational evaluations, where workers reported hospitalizations for cardiovascular events. All reported events were then verified against hospital discharge records transmitted to the employing company and subsequently to the occupational clinic. In the occupational health context, major cardiovascular events requiring hospitalization are systematically documented because they generate mandatory sick leave, medical reassessment, and potential work restrictions or job reassignment. Final event classification was therefore based on hospital discharge diagnoses according to treating physician criteria, not on self-report alone.
Covariates such as age and sex (classified as male or female) were also considered. Alcohol consumption and smoking habits in the last 30 days were recorded in binary format (“yes” or “no”), consistent with standardized occupational health surveillance protocols in Peru. AC, total cholesterol, and triglycerides were evaluated as continuous variables for the main analysis. However, for purely descriptive purposes and to facilitate clinical interpretation by decision-makers, these variables are also presented categorized according to cutoff points established in clinical guidelines.
For descriptive population characterization, abdominal obesity was defined as AC ≥ 88 cm in women and ≥ 102 cm in men. Triglycerides were considered elevated with values ≥ 150 mg/dL, and hypercholesterolemia was defined as total cholesterol ≥ 200 mg/dL. It is important to emphasize that these categorizations were used solely for sample description (Table 1), while association analyses preserved the continuous nature of these variables through modeling with restricted cubic splines (RCS), thus avoiding the loss of information and statistical power inherent to dichotomization, as we will elaborate in the statistical analysis section.
 Click to view |
Table 1. General Characteristics in the Worker
Sample |
Procedures
Participant evaluation was developed in several stages, beginning with registration of personal and occupational data in clinical records, which allowed the formation of complete clinical files for longitudinal follow-up.
Subsequently, a general physical examination was performed that included measurement of blood pressure, BMI, and AC. Blood pressure was recorded using a digital sphygmomanometer (Omron), performing three successive measurements with 5-min intervals. Evaluations were carried out with the participant seated, with straight back and feet flat on the floor. The arm was positioned at heart level, and the final value was obtained by averaging the last two readings of systolic and diastolic pressure, expressed in mm Hg.
BMI was estimated from weight and height measurements using calibrated equipment (scale and stadiometer). Measurements were performed with workers barefoot and wearing light clothing. BMI calculation was performed using the standard formula: BMI = weight (kg)/height2 (m2). AC was measured with a measuring tape positioned between the lower edge of the last rib and the upper edge of the iliac crests. The value was recorded in cm.
Subsequently, biochemical parameters were evaluated through laboratory analysis. Participants were instructed to fast for at least 8 h before sample collection. Blood draws were performed under aseptic conditions, following biosafety protocols, and were processed in an accredited clinical laboratory. Fasting glucose, triglycerides, and total cholesterol values were obtained.
Finally, a structured interview was applied to gather health-related habits, such as recent alcohol and tobacco consumption. All information was recorded on a secure electronic platform. It is important to note that data were collected as part of routine medical care, without research purposes at origin.
Statistical analysis
For statistical analysis, data were initially recorded in Microsoft Excel spreadsheets and subsequently subjected to a rigorous process of cleaning, debugging, and validation to ensure information quality. All analyses were performed using RStudio software (version 4.1.0 or higher), supported by the survival, rms, and msm packages.
Participants with incomplete baseline data on exposure variables (blood pressure, glucose, or anthropometric parameters) or covariates were excluded, resulting in a complete-case analysis. For time-to-event analyses, participants who discontinued employment or were lost to follow-up without experiencing a cardiovascular event were censored at their last evaluation date.
A descriptive analysis of baseline cohort characteristics was conducted. Categorical variables were summarized using absolute frequencies and proportions, while continuous variables were described using measures of central tendency (mean) and dispersion (standard deviation (SD)), following normality assessment.
To identify associations between combinations of obesity, hypertension, and diabetes with cardiovascular outcomes, Cox regression models for time-to-event data were used. Crude HR (cHR) and adjusted HR (aHR) were estimated, along with their respective 95% confidence intervals (Cis). The proportional hazards assumption was evaluated using the Schoenfeld residuals test, both globally and for each covariate. No significant violations were detected (global test P = 0.133), supporting the validity of the Cox regression estimates.
Variable selection for the adjusted model was based on a directed acyclic graph (DAG) constructed based on prior knowledge and biological plausibility. This causal analysis identified as minimal sufficient confounders for the adjustment set: sex, age, smoking status and alcohol consumption, total cholesterol, and triglycerides. Other potentially relevant variables were not included in the model as they were identified as mediators in the causal pathway between exposures and outcome, which would have introduced overadjustment bias. Specifically, AC was not included due to its high multicollinearity with BMI (variance inflation factor > 10), with BMI being the primary anthropometric measure selected.
The final model included sex as a binary categorical variable, while age, total cholesterol, and triglycerides were modeled using RCS with three knots, allowing capture of possible non-linear relationships with the outcome without assuming arbitrary cutoff points or strictly linear relationships.
Ethical considerations
This study was conducted following appropriate ethical procedures, having secured the necessary institutional permissions from the clinic to access and utilize the workers’ database. The research protocol received formal approval from the Institutional Review Board of Toribio Rodriguez de Mendonza University of Amazonas, Peru.
Data protection protocols were rigorously implemented throughout the study. The clinic provided completely deidentified datasets, with all personal identifiers removed to ensure participant anonymity. This approach safeguards individual privacy and maintains strict confidentiality standards, which are essential principles in health research ethics. Database access was restricted solely to the principal investigator, thereby reducing potential risks of confidentiality breaches. To promote scientific transparency and reproducibility, the anonymized dataset has been made publicly available [12].
| Results | ▴Top |
The study included a cohort of 10,300 workers without a history of cardiovascular disease at baseline. A total of 79,660 records were identified in the occupational clinic database. Of these, 67,611 were excluded due to missing follow-up time, and 56 were excluded due to prevalent cardiovascular disease at baseline, leaving 11,993 eligible participants. After excluding 1,693 individuals with missing anthropometric data, the final analytical sample comprised 10,300 workers without a history of cardiovascular disease at baseline (Fig. 1).
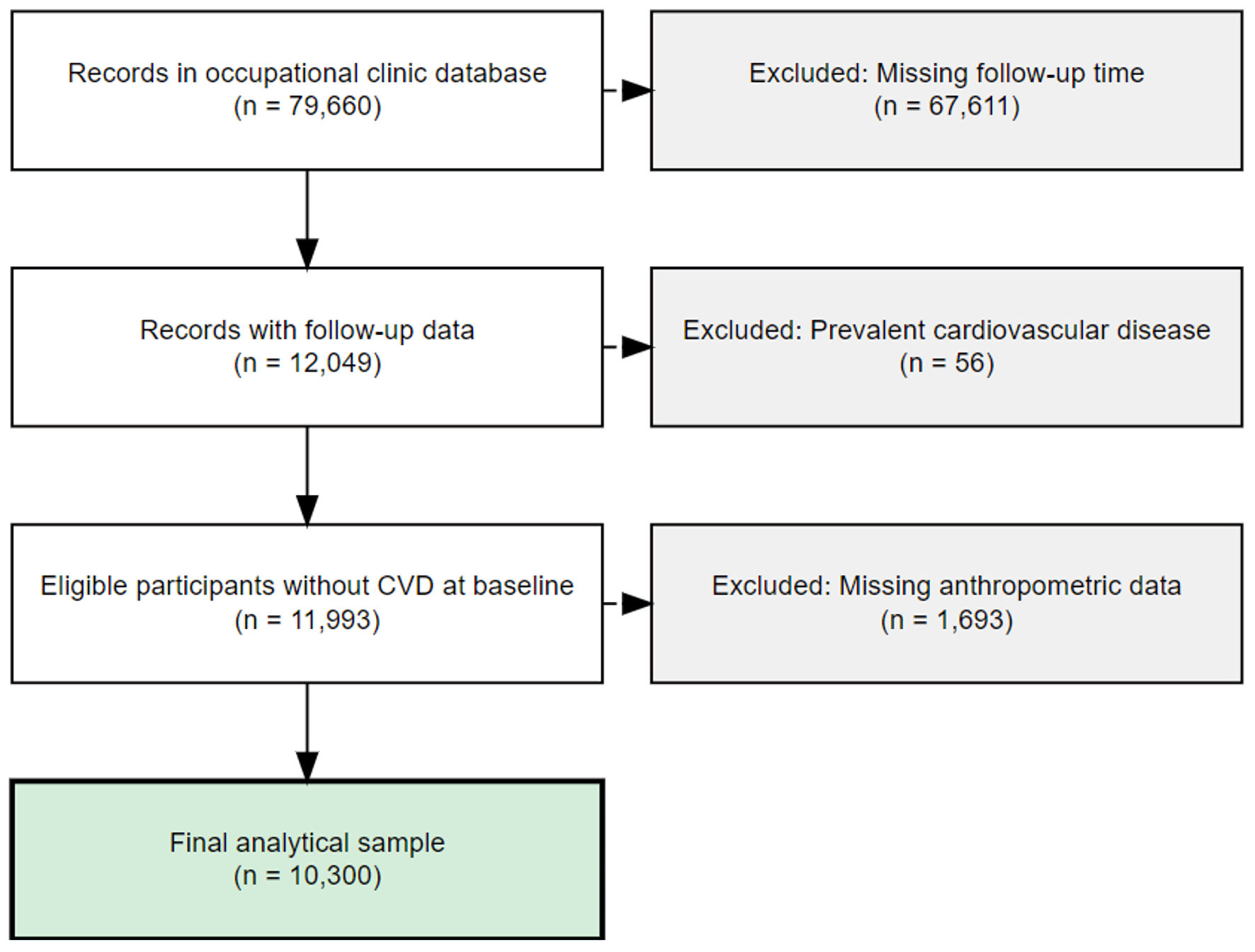 Click for large image |
Figure 1. Flow diagram of participant selection. CVD: cardiovascular disease. |
Baseline characteristics of the study population are presented in Table 1. The majority were men (84.57%), and the mean age was 37.17 years (SD: 11.53). Additionally, 95.60% of participants were in the 18 to 59 year age range. Regarding lifestyle habits, 41.45% (n = 4,269) reported tobacco use in the last 30 days and 50.07% (n = 5,157) reported alcohol consumption.
From a metabolic standpoint, mean BMI was 27.18 kg/m2 (SD: 4.02), while AC had a mean value of 91.15 cm (SD: 10.41). Mean systolic blood pressure was 110.93 mm Hg (SD: 12.14) and diastolic 71.68 mm Hg (SD: 13.88). Fasting glucose had a mean value of 94.11 mg/dL (SD: 21.24), triglycerides averaged 145.36 mg/dL (SD: 82.55), and total cholesterol 196.32 mg/dL (SD: 37.28).
Regarding the combination of cardiometabolic triad components, 2,509 participants (24.36%) presented obesity only, 115 (1.12%) diabetes only, and 216 (2.10%) hypertension only. Additionally, 90 individuals (0.87%) were identified with obesity and diabetes, 17 (0.17%) with obesity and hypertension, 17 (0.17%) with diabetes and hypertension, and 34 (0.33%) with all three conditions present simultaneously.
Incidence and risk of the metabolic triad
A progressive increase in event risk was observed as the number of metabolic triad components increased. The reference group, individuals without any of these components, recorded the lowest incidence (1.30 per 1,000 person-years; 95% CI: 0.77 - 1.84) (Table 2).
Click to view |
Table 2. Incidence and Cardiovascular Risk by
Metabolic Triad Categories |
Regarding hazard level, among individual factors, diabetes alone showed the highest risk in the multivariate analysis (aHR: 4.24; 95% CI: 1.36 - 13.35), followed by obesity alone (aHR: 1.45; 95% CI: 0.68 - 3.10) and hypertension alone (aHR: 1.17; 95% CI: 0.32 - 4.24). In two-component combinations, the coexistence of obesity and diabetes presented the highest risk (aHR: 6.34; 95% CI: 1.73 - 23.27), followed by diabetes and hypertension (aHR: 5.86; 95% CI: 1.47 - 23.39). Finally, those who presented the complete metabolic triad had the highest risk, almost 11 times greater than the reference group (aHR: 10.87; 95% CI: 2.81 - 42.06) (Fig. 2).
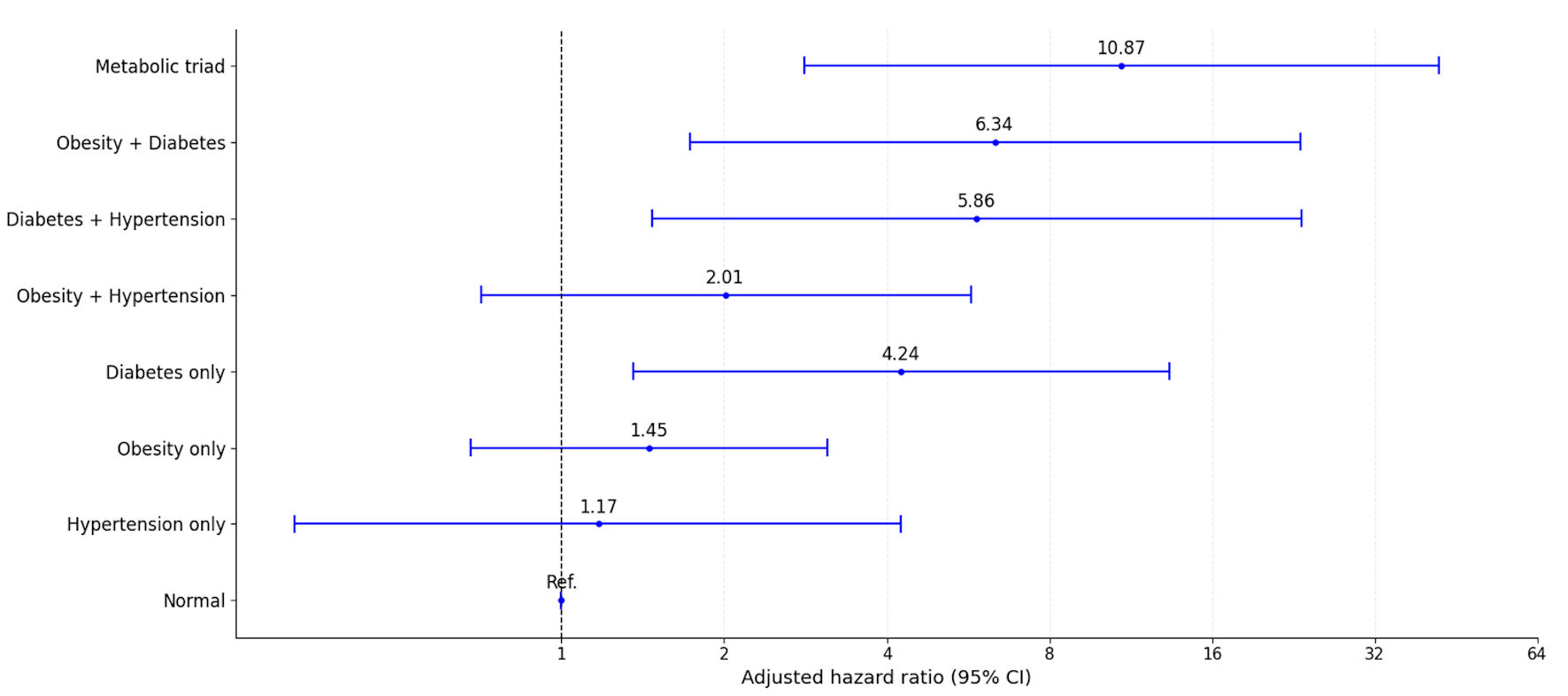 Click for large image |
Figure 2. Adjusted hazard ratios (aHR) for cardiovascular events according to metabolic triad categories. CI: confidence interval. |
| Discussion | ▴Top |
Main findings
In this Peruvian occupational cohort, a progressive increase in event risk was evidenced with each additional component of the metabolic triad. The reference group, without obesity, hypertension, or diabetes, presented the lowest incidence (1.30 per 1,000 person-years, aHR = 1). The simultaneous combination of the three conditions was associated with an incidence of 34.94 per 1,000 person-years and with an adjusted risk almost 11 times higher (aHR: 10.87; 95% CI: 2.81 - 42.06).
Among individual factors, diabetes was the main determinant of cardiovascular risk (aHR: 4.24; 95% CI: 1.36 - 13.35), surpassing obesity and hypertension. It is noteworthy that combinations including diabetes: obesity + diabetes (aHR: 6.34; 95% CI: 1.73 - 23.27) and diabetes + hypertension (aHR: 5.86; 95% CI: 1.47 - 23.39) concentrated the highest risks, reinforcing its central role as a driver within the metabolic triad in the working population.
Comparison with international and regional literature
At the regional level, the PURE-South America substudy (Argentina, Brazil, Chile, and Colombia) quantified the population contribution of modifiable factors to CVD: hypertension 18.7%, abdominal obesity 15.4%, and diabetes 5.3%, prioritizing precisely the three components evaluated here and supporting their relevance for the region [8]. In our study, cardiovascular risk increased consistently with each additional component of the metabolic syndrome, reaching its highest level when obesity, hypertension, and type 2 diabetes coexisted, with type 2 diabetes being the component associated with the most marked risk increase. These findings are concordant with scientific evidence that has documented that diabetes increases approximately 1.5 to 2 times the risk of major cardiovascular events compared to non-diabetic individuals [13], and contemporary analyses that reveal 2 to 4 times higher risks of mortality and cardiovascular events in patients with diabetes compared to the general population [7].
In our analysis, the association with hypertension was not statistically significant; however, available evidence indicates a continuous relationship between blood pressure and cardiovascular comorbidity risk starting at 115/75 mm Hg [14]. Additionally, trials demonstrate that reducing systolic blood pressure by 10 mm Hg proportionally decreases major events [15], supporting causality and suggesting that high dichotomous thresholds may underestimate risk in younger populations like ours.
Regarding obesity, our estimate is consistent with meta-analyses showing that for every 5 kg/m2 increase in BMI, coronary heart disease risk increases by approximately 27% and stroke risk by about 18% [16]. Congruently, a meta-analysis of 21 cohorts estimated that, compared to normal weight, overweight is associated with relative risk (RR) = 1.32 and obesity with RR = 1.81 for coronary heart disease [17]. Additionally, a continuous relationship between BMI and CVD has been demonstrated: for every -2 kg/m2, the risk of ischemic heart disease and stroke was reduced by 11-12% [18].
In our cohort, the comorbidity pattern showed that the highest risks were concentrated in dyads that include diabetes (obesity + diabetes; diabetes + hypertension) and, with greater intensity, in the obesity + diabetes + hypertension triad. At the syndrome level, it is associated with approximately double the risk of cardiovascular events and higher total mortality [19]. Additionally, a national cohort confirms that the co-occurrence of diabetes and hypertension carries risks superior to those of each condition separately, as well as higher total and cardiovascular mortality compared to presenting only one of them [20].
Finally, UK Biobank studies show that people with diabetes and normal BMI may present higher cardiovascular mortality than obese individuals without diabetes, emphasizing that chronic hyperglycemia can dominate the risk profile above total body mass [21]. This finding is coherent with our central result: all combinations with higher risk included diabetes, and maximum risk was observed when type 2 diabetes, arterial hypertension, and obesity coexist.
Metabolic risk multiplying mechanisms
Diabetes positions itself as the central node of risk when it coexists with obesity and/or hypertension. Sustained hyperglycemia activates the advanced glycation end products-receptor for advanced glycation end products (AGEs-RAGE) axis, promotes oxidative stress and endothelial activation/dysfunction and proinflammatory pathways (chronic low-grade inflammation) that accelerate atherogenesis and favor vulnerable plaques [22, 23]. Added to this is diabetic dyslipidemia (increased very-low-density lipoprotein (VLDL)/triglyceride-rich lipoproteins (TRL), small dense low-density lipoprotein (LDL), and decreased functional high-density lipoprotein (HDL)) and increased prothrombotic tone, configuring a terrain conducive to acute arterial events [24, 25].
Excessive adiposity increases sympathetic activity, activates the renin-angiotensin-aldosterone system (RAAS), facilitates sodium retention and renal compression by ectopic fat, and elevates oxidative stress; thereby promoting elevated blood pressure and arterial stiffness over a vulnerable endothelium [26]. At the population level, blood pressure relates continuously to the risk of multiple CVD presentations, and its reduction by 10 mm Hg proportionally decreases events, supporting causality [15, 27]. For its part, obesity is independently associated with higher CVD risk and contributes to the development of AH, dysglycemia, and other metabolic intermediaries [16]. Together, the convergence of hyperglycemia, hemodynamic load, and oxidative stress multiplies risk, coherent with what was observed in our cohort (doublets that include diabetes and a maximum in the triad).
Clinical implications
Practical implementation of the observed results requires prioritizing, within occupational surveillance, those who concentrate the most potential benefit: 1) workers with the triad (very high risk); and 2) those presenting diabetes plus a second component (high risk). In these subgroups, it is advisable to intensify follow-up frequency (closer clinical and laboratory controls), ensure blood pressure and glycemia targets according to current guidelines, and implement timely therapeutic escalation (e.g., combination of antihypertensive drugs when appropriate; and, in diabetes, use of agents with cardiovascular benefit such as sodium-glucose cotransporter-2 inhibitors (SGLT2i) and/or glucagon-like peptide 1 (GLP-1) agonists in the presence of high risk or established CVD), along with lipid optimization according to risk [28, 29]. These lines are congruent with evidence that blood pressure reduction is associated with fewer events across a broad baseline blood pressure range and with data describing a continuous relationship between blood pressure and multiple CVD presentations [15, 27]. At the regional level, prioritization of hypertension, obesity, and diabetes in prevention strategies is consistent with the attributable burden described for South America [30], reinforcing the relevance of focusing resources on these components within the work environment.
At the organizational level, integrating risk stratification into occupational clinical record flows (standardized records of blood pressure and BMI; glucose/glycosylated hemoglobin (HbA1c) and lipid profile when available) and activating alerts for cases with diabetes and combinations of two or three components, allows managing prevention selectively and measurably. These actions should be accompanied by workplace interventions, such as reducing sitting time through standing stations/active breaks and promoting physical activity during the workday. These measures are supported by reviews and meta-analyses showing sustained decreases in sedentary time and favorable associations with mortality [31, 32]. Although the effect on hard outcomes in workplace contexts requires follow-up, the direction of evidence supports their implementation as part of a multicomponent package. At the policy level, these findings support the inclusion of metabolic triad screening as a standard component of occupational health regulations, with particular emphasis on early diabetes detection given its central role in cardiovascular risk. Health systems could consider establishing referral pathways and performance indicators for occupational clinics based on the proportion of high-risk workers identified and effectively managed.
Strengths and limitations
This study presents significant methodological strengths that include a large and longitudinal cohort of workers with 8 years of follow-up in a Latin American context scarcely explored in the literature; major cardiovascular outcomes (incident acute myocardial infarction and stroke) with rigorous exclusion of prevalent cardiovascular disease; a mutually exclusive classification of risk triad combinations that allows precise quantification of the cardiovascular risk gradient; and a parsimonious adjustment model, guided by a directed acyclic graph, which incorporates spline functions and minimizes the risk of overfitting. These methodological characteristics reinforce the study’s internal validity by strategically leveraging the periodicity inherent to occupational medical surveillance to ensure temporal consistency of measurements.
However, the study presents limitations that should be considered in interpreting results, including dichotomization of blood pressure and BMI that entails loss of information and possible underestimation of continuous associations; diabetes definition based exclusively on fasting glucose, without incorporating HbA1c or oral glucose tolerance test, which may result in case misclassification; low number of cases in some triad combinations (e.g., certain doublets and the triad), translating to imprecise estimates with wide confidence intervals; and residual confounding by unmeasured factors. Specifically, information on dietary patterns, physical activity levels, and medication use (antihypertensives, hypoglycemic agents, or lipid-lowering drugs) was not available in the occupational surveillance records. These factors may influence both the development of metabolic conditions and cardiovascular outcomes, potentially biasing effect estimates. While our analysis was guided by a directed acyclic graph to identify minimal sufficient adjustment sets, the observational nature of this study precludes definitive causal inference, and associations should be interpreted as predictive rather than strictly causal. Despite these methodological limitations, the findings provide valuable evidence on the risk gradient associated with the metabolic triad and establish a solid foundation for future research.
On the other hand, the predominance of male participants (84.57%) may limit the generalizability of findings to female workers. However, this distribution is consistent with the composition of formal private employment in Peru, where approximately 64% of workers are men, with even higher male predominance in sectors such as mining, construction, and manufacturing commonly served by occupational clinics [33]. Finally, additionally, potential selection bias cannot be ruled out, as the inclusion of workers depended on the completeness of data determined by employer-requested evaluations. Workers with incomplete records may differ systematically from those included, potentially affecting generalizability. However, this limitation is inherent to secondary data analyses from occupational surveillance systems.
Conclusions
This study demonstrates that the coexistence of obesity, hypertension, and diabetes progressively amplifies cardiovascular risk in working populations, with diabetes acting as the central driver. These findings carry direct implications for occupational health practice: systematic screening for the metabolic triad components should be incorporated into routine workplace evaluations, with particular emphasis on early diabetes detection. Risk stratification protocols that prioritize workers with diabetes (alone or in combination with obesity or hypertension) can optimize resource allocation and enable targeted interventions, including intensified follow-up, therapeutic escalation, and workplace-based lifestyle programs such as active breaks and healthy food options.
Given that the metabolic triad components are easily measurable with minimal laboratory requirements, this approach is particularly suited for implementation in low- and middle-income countries, where occupational health infrastructure may serve as an accessible platform for cardiovascular prevention. These findings may inform similar screening and prevention programs across Latin America and other regions facing comparable epidemiological transitions and resource constraints.
Acknowledgments
Special thanks to the members of Universidad Nacional Toribio Rodriguez de Mendoza de Amazonas (UNTRM), Amazonas, Peru, for their support and contributions throughout the completion of this research.
Financial Disclosure
This study was financed by Vicerectorado de Investigacion de la Universidad Nacional Toribio Rodriguez de Mendoza de Amazonas.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Since this is a secondary data analysis, informed consent was not required.
Author Contributions
Lupita Ana Maria Valladolid-Sandoval: methodology, data curation, writing - original draft, writing - review and editing. Jhosmer Ballena-Caicedo: conceptualization, investigation, methodology, software, writing - original draft, writing - review and editing. Fiorella E. Zuzunaga-Montoya: software, investigation, data curation, methodology, funding acquisition, supervision, writing - original draft, writing - review and editing. Victor Juan Vera-Ponce: conceptualization, investigation, formal analysis, methodology, resources, writing - original draft, writing - review and editing.
Data Availability
The data supporting the findings of this study can be accessed through the following link: https://figshare.com/articles/dataset/b_Database_Ocupacional_b/27098296?file=49391110.
| References | ▴Top |
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM,
Barengo NC, et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update
From the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982-3021.
doi pubmed - Joseph P, Lanas F, Roth G, Lopez-Jaramillo P, Lonn E, Miller V, Mente
A, et al. Cardiovascular disease in the Americas: the epidemiology of cardiovascular disease and
its risk factors. Lancet Reg Health Am. 2025;42:100960.
doi pubmed - Alhuneafat L, Al Ta'ani O, Arriola-Montenegro J, Al-Ajloun YA, Naser
A, Chaponan-Lavalle A, Ordaya-Gonzales K, et al. The burden of cardiovascular disease in Latin
America and the Caribbean, 1990-2019: An analysis of the global burden of disease study. Int J
Cardiol. 2025;428:133143.
doi pubmed - The Lancet Regional Health - Americas. Cardiovascular disease:
addressing poverty is key. Lancet Reg Health Am. 2025;42:101029.
doi pubmed - Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, et
al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52
countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937-952.
doi pubmed - Oguz A, Kilickap M, Gulec S, Altuntas Y, Karsidag K, Temizhan A,
Tumerdem BC, et al. Risk of cardiovascular events in patients with metabolic syndrome: Results
of a population-based prospective cohort study (PURE Turkey). Anatol J Cardiol.
2020;24(3):192-200.
doi pubmed - Rawshani A, Rawshani A, Franzen S, Sattar N, Eliasson B, Svensson AM,
Zethelius B, et al. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2
Diabetes. N Engl J Med. 2018;379(7):633-644.
doi pubmed - Lopez-Jaramillo P, Lopez-Lopez JP. Cardiovascular risk factors and
death in South America. Clin Investig Arterioscler. 2023;35(4):195-200.
doi pubmed - Carrillo-Larco RM, Altez-Fernandez C, Pacheco-Barrios N, Bambs C,
Irazola V, Miranda JJ, Danaei G, et al. Cardiovascular Disease Prognostic Models in Latin
America and the Caribbean: A Systematic Review. Glob Heart. 2019;14(1):81-93.
doi pubmed - Kreutz R, Brunstrom M, Burnier M, Grassi G, Januszewicz A, Muiesan
ML, Tsioufis K, et al. 2024 European Society of Hypertension clinical practice guidelines for
the management of arterial hypertension. Eur J Intern Med. 2024;126:1-15.
doi pubmed - American Diabetes Association Professional Practice Committee. 2.
Diagnosis and Classification of Diabetes: Standards of Care in Diabetes-2025. Diabetes Care.
2025;48(1 Suppl 1):S27-S49.
doi pubmed - Vera Ponce VJ. Database Ocupacional [Internet]. figshare; 2024
[citado el 24 de septiembre de 2024]. p. 8073963 Bytes.
doi - Ahmad A, Lim LL, Morieri ML, Tam CH, Cheng F, Chikowore T,
Dudenhoffer-Pfeifer M, et al. Precision prognostics for cardiovascular disease in Type 2
diabetes: a systematic review and meta-analysis. Commun Med (Lond). 2024;4(1):11.
doi pubmed - Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective
Studies C. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis
of individual data for one million adults in 61 prospective studies. Lancet.
2002;360(9349):1903-1913.
doi pubmed - Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J,
Chalmers J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a
systematic review and meta-analysis. Lancet. 2016;387(10022):957-967.
doi pubmed - Global Burden of Metabolic Risk Factors for Chronic Diseases C, Lu Y,
Hajifathalian K, Ezzati M, Woodward M, Rimm EB, Danaei G. Metabolic mediators of the effects of
body-mass index, overweight, and obesity on coronary heart disease and stroke: a pooled analysis
of 97 prospective cohorts with 1.8 million participants. Lancet. 2014;383(9921):970-983.
doi pubmed - Bogers RP, Bemelmans WJ, Hoogenveen RT, Boshuizen HC, Woodward M,
Knekt P, van Dam RM, et al. Association of overweight with increased risk of coronary heart
disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21
cohort studies including more than 300 000 persons. Arch Intern Med.
2007;167(16):1720-1728.
doi pubmed - Ni Mhurchu C, Rodgers A, Pan WH, Gu DF, Woodward M, Asia Pacific
Cohort Studies C. Body mass index and cardiovascular disease in the Asia-Pacific Region: an
overview of 33 cohorts involving 310 000 participants. Int J Epidemiol.
2004;33(4):751-758.
doi pubmed - Mottillo S, Filion KB, Genest J, Joseph L, Pilote L, Poirier P,
Rinfret S, et al. The metabolic syndrome and cardiovascular risk a systematic review and
meta-analysis. J Am Coll Cardiol. 2010;56(14):1113-1132.
doi pubmed - Yen FS, Wei JC, Chiu LT, Hsu CC, Hwu CM. Diabetes, hypertension, and
cardiovascular disease development. J Transl Med. 2022;20(1):9.
doi pubmed - Brown OI, Drozd M, McGowan H, Giannoudi M, Conning-Rowland M, Gierula
J, Straw S, et al. Relationship Among Diabetes, Obesity, and Cardiovascular Disease Phenotypes:
A UK Biobank Cohort Study. Diabetes Care. 2023;46(8):1531-1540.
doi pubmed - Ramasamy R, Shekhtman A, Schmidt AM. RAGE/DIAPH1 and atherosclerosis
through an evolving lens: Viewing the cell from the "Inside - Out". Atherosclerosis.
2024;394:117304.
doi pubmed - Zhou M, Zhang Y, Shi L, Li L, Zhang D, Gong Z, Wu Q. Activation and
modulation of the AGEs-RAGE axis: Implications for inflammatory pathologies and therapeutic
interventions - A review. Pharmacol Res. 2024;206:107282.
doi pubmed - Hirano T. Pathophysiology of Diabetic Dyslipidemia.
J Atheroscler Thromb. 2018;25(9):771-782.
doi pubmed - Li Z, Zhang J, Ma Z, Zhao G, He X, Yu X, Fu Q, et al. Endothelial YAP
Mediates Hyperglycemia-Induced Platelet Hyperactivity and Arterial Thrombosis. Arterioscler
Thromb Vasc Biol. 2024;44(1):254-270.
doi pubmed - Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity-induced
hypertension: interaction of neurohumoral and renal mechanisms. Circ Res.
2015;116(6):991-1006.
doi pubmed - Rapsomaniki E, Timmis A, George J, Pujades-Rodriguez M, Shah AD,
Denaxas S, White IR, et al. Blood pressure and incidence of twelve cardiovascular diseases:
lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people.
Lancet. 2014;383(9932):1899-1911.
doi pubmed - American Diabetes Association Professional Practice Committee. 10.
Cardiovascular Disease and Risk Management: Standards of Care in Diabetes-2025. Diabetes Care.
2025;48(1 Suppl 1):S207-S238.
doi pubmed - American Diabetes Association Professional Practice C. Summary of
Revisions: Standards of Care in Diabetes-2025. Diabetes Care. 2025;48(1 Suppl 1):S6-S13.
doi pubmed - Lopez-Jaramillo P, Joseph P, Lopez-Lopez JP, Lanas F, Avezum A, Diaz
R, Camacho PA, et al. Risk factors, cardiovascular disease, and mortality in South America: a
PURE substudy. Eur Heart J. 2022;43(30):2841-2851.
doi pubmed - Shrestha N, Kukkonen-Harjula KT, Verbeek JH, Ijaz S, Hermans V,
Pedisic Z. Workplace interventions for reducing sitting at work. Cochrane Database Syst Rev.
2018;6(6):CD010912.
doi pubmed - Ekelund U, Tarp J, Steene-Johannessen J, Hansen BH, Jefferis B,
Fagerland MW, Whincup P, et al. Dose-response associations between accelerometry measured
physical activity and sedentary time and all cause mortality: systematic review and harmonised
meta-analysis. BMJ. 2019;366:l4570.
doi pubmed - Coaguila JP. Tendencias del empleo formal privado de Peru: un
analisis con planilla electronica (2008-2018). Rev Latinoam Desarro Economico.
2019;17(32):34-56.
doi
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Endocrinology and Metabolism is published by Elmer Press Inc.