| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Original Article
Volume 000, Number 000, January 2025, pages 000-000

Prevalence of Self-Reported Halitosis in Individuals With Type 1 and Type 2 Diabetes Mellitus: A Cross-Sectional Study
Mohammed S. Almayoufa, f, Saleh S. Alorainib, Khaled H. Aburishehc, Muhammad Mujammamic, d, Hamad N. AlBagiehe, Hamad A. Alzomanb, f
aGraduate Program in Periodontics, Department of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh, Saudi Arabia
bDepartment of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh, Saudi Arabia
cUniversity Diabetes Center, King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia
dDepartment of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia
eDepartment of Oral Medicine and Diagnostic Sciences, College of Dentistry, King Saud University, Riyadh, Saudi Arabia
fCorresponding Author: Hamad A. Alzoman, Department of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh, Saudi Arabia; Mohammed S. Almayouf, Graduate Program in Periodontics, Department of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh, Saudi Arabia
Manuscript submitted November 20, 2024, accepted January 17, 2025, published online January 24, 2025
Short title: Self-Reported Halitosis in TDM1 and TDM2
doi: https://doi.org/10.14740/jem1050
| Abstract | ▴Top |
Background: Diabetes mellitus (DM) is a well-known metabolic disorder that leads to multiple oral complications, including increased caries incidence, periodontal breakdown, periapical abscesses, and delayed wound healing. Oral malodor is influenced by local (intraoral) and systemic (extraoral) factors. DM is believed to have a direct influence on both intra and extra oral halitosis. The aim of the study was to evaluate the prevalence of self-reported halitosis among diabetic individuals and compare it between type 1 and type 2 diabetes.
Methods: A cross-sectional online survey consisting of 34 questions was used. The survey collected demographic, medical and lifestyle data, as well as halitosis-related parameters. The survey was validated by two experts and piloted with 30 participants to ensure clarity and reliability. The targeted sample consisted of individuals with type 1 DM (group I), type 2 DM (group II), and a control group of healthy subjects (group III).
Results: A total of 632 surveys were analyzed, with 12 subjects excluded due to reported loss of smelling ability. Halitosis was self-reported by 50.7%, 48.0% and 28.0% of groups I, II and III, respectively. Subjects with DM reported a higher intensity of halitosis (P value = 0.005), with more than 65% of respondents reported smelling ability score more than 8 out of 10, and the subjects with diabetes reported significantly less smelling ability score. Only 1.7% of subjects with DM were informed about their halitosis by a healthcare provider.
Conclusions: DM demonstrates a significant correlation with halitosis prevalence and intensity, with similar outcomes observed in individuals with type 1 and type 2 DM. The reported reduced smelling ability in patients with DM may lead to an underestimation of self-reported halitosis. Moreover, insufficient communication from healthcare providers further exacerbates this issue.
Keywords: Oral malodor; Self-reported halitosis; Type 1 diabetes; Type 2 diabetes; Oral health; Olfaction
| Introduction | ▴Top |
The term halitosis refers to an unpleasant odor that originates during exhalation. The source of this offensive smell could be either intraoral or extraoral [1]. Globally, about 50% of individuals suffer from halitosis to varying degrees [2]. In some studies, the prevalence of halitosis has been reported to reach 60% of the population [3]. In a systematic review by Silva et al, self-reported halitosis prevalence ranges from 24.4% to 43.4% [4].
Given the widespread prevalence of halitosis, it is important to understand the different factors contributing to its development. In general, the source of halitosis could be either extraoral, such as gastrointestinal problems, respiratory tract infection, diabetes mellitus (DM), or renal and hepatic diseases [5], or intraoral. Approximately 85% of the reported cases arise from intraoral sources associated with periodontal disease, caries, odontogenic infections, tongue coating, and faulty restorations [6].
DM is believed to contribute to the development of extraoral halitosis. The levels of volatile organic compounds, including phenol, indole, ammonia, and acetone in the exhaled air of diabetic subjects are elevated, leading to a noticeable odor. These compounds are considered end products of the metabolic processes that lead to oral malodor [7, 8].
The altered metabolic processes in patients with DM lead to increased circulating ketone bodies in the bloodstream [9]. Several studies have reported elevated levels of acetone, a ketone body commonly associated with prolonged starvation, ketogenic diets, or bariatric surgery [9, 10]. Furthermore, the levels of exhaled acetone concentrations in patients with DM were observed to be higher than those in healthy subjects [11].
In addition, long-term diabetes leads to impaired immunity, delayed healing, and soft tissue infections [12, 13]. Consequently, DM is linked to an increased risk of oral diseases such as periodontal disease and dental caries [14]. Many oral bacteria, especially gram-negative anaerobic species, are found in greater numbers in the subgingival biofilm of deep periodontal pockets and on the dorsum of the tongue in individuals with diabetes. These bacteria produce volatile sulfur compounds (VSCs), such as methanethiol, hydrogen sulfide, and dimethyl sulfide, which are responsible for intraoral halitosis [15, 16].
Given the strong connection between oral bacteria, diabetes, and halitosis, it is essential to assess the prevalence of halitosis and its related factors in patients with DM. However, there are limited studies in the literature evaluating the relationship between DM and self-reported halitosis. To our knowledge, no existing study specifically assesses self-reported halitosis in both subjects with type 1 and type 2 DM. It has been hypothesized that the prevalence and intensity of halitosis will be significantly higher in subjects with DM compared to non-diabetic subjects. Thus, the aim of this study is to evaluate the prevalence of self-reported halitosis among diabetic individuals and compare this prevalence between individuals with type 1 and type 2 diabetes.
| Materials and Methods | ▴Top |
Ethical consideration
Ethical approval was obtained from both the Institutional Review Board (IRB) (E-19-4253) and the College of Dentistry Research Center (CDRC), at King Saud University, Riyadh, Saudi Arabia. In accordance with ethical guidelines following the Helsinki Declaration, informed consent was obtained from all participants, and participation in the study was entirely voluntary.
Study sample and survey design
This cross-sectional study targeted both subjects with type 1 and type 2 DM. A comprehensive survey questionnaire was developed to assess the prevalence, knowledge, and awareness of halitosis among participants with DM.
For the survey construction, the literature was scanned, and the initial survey consisted of 63 questions. The survey was designed to cover seven domains, including demographic data, medical and lifestyle information, dental condition, halitosis, oral hygiene, smell ability, and coronavirus disease 2019 (COVID-19)-related complications. The questionnaire underwent validation using established methods, including content validity by two experts, face validity through pilot testing, and test-retest reliability.
Content validity was performed by two experts who evaluated the survey using a validation form to judge the relevance and clarity of each item. Following expert discussions, the questions were shortlisted to 34, with 29 redundant or irrelevant questions being merged or removed. Subsequently, the content validity index (CVI) was calculated (scale-level content validity index (average) (S-CVI avg) = 1, scale-level content validity index (universal agreement, average) (S-CVI UA avg) = 1) [17]. Face validity was conducted to evaluate the clarity of the questions by interviewing 30 volunteers who participated in pilot testing and provided feedback. Based on their feedback, six questions were revised. The final questionnaire, comprising 34 questions, was tested for reliability. Thirty participants completed the survey and were re-invited to answer the questionnaire again after 14 days. The answers from the first and second rounds were recorded, and test-retest reliability was assessed using the intraclass correlation coefficient (ICC). The ICC score was 0.85, which is considered good agreement [18].
A final validated questionnaire comprising 34 questions was distributed. An online template was designed to ensure that participants answered all 34 questions. Participants were invited to participate voluntarily in our study through email and social media. The survey was conducted between November 2022 and October 2023. Inclusion criteria included individuals aged 18 and above with type 1 or type 2 diabetes, along with a control group of non-diabetic individuals.
The study subjects were grouped into three categories as follows: group I (type 1 diabetes), group II (type 2 diabetes), and group III (non-diabetic).
Outcome measures
The survey was structured to assess the relationship between diabetes (type 1 and type 2) and related factors on self-reported knowledge and awareness of halitosis.
Statistical analysis
Recorded data were analyzed using the Statistical Package for Social Sciences program for Windows (IBM SPSS Statistics Version 26, Chicago, IL, USA). Descriptive data, including percentages and frequencies, were calculated. The difference between the mean of the groups was evaluated using analysis of variance (ANOVA). If the difference between the groups was significant, a post hoc test was performed. Additionally, the correlation between different variables was assessed using Pearson’s correlation coefficient to determine relationships between variables, such as hemoglobin A1c (HbA1c) levels and halitosis scores, and the duration of diabetes and awareness of halitosis. A P value of less than 0.05 was considered statistically significant.
| Results | ▴Top |
A total of 644 surveys were received, of which 12 subjects were excluded from the analysis due to reported loss of smelling ability as this condition would interfere with the accurate self-reporting of halitosis. Therefore, 632 responses were analyzed and included in the study. The mean age of the entire sample was 39.8 (± 14.01) years. Among these participants, there were 273 (43.1%) males and 359 (56.9%) females, with 282 (44.6%) identified as subjects with DM and 350 (55.4%) as healthy subjects. The analysis revealed that the participants were distributed into three groups as follows: group I (type 1 diabetes, 138 participants), group II (type 2 diabetes, 144 participants), and group III (non-diabetic, 350 participants). Detailed demographic information is provided in Table 1.
 Click to view | Table 1. Demographic Characteristics of Participant |
The overall halitosis prevalence among the respondents was 37.5%, while subjects with DM showed a higher rate of 49.3%. The prevalence of halitosis varied significantly among the different groups, with rates of 50.7%, 48.0%, and 28.0% observed in group I, group II, and group III, respectively (P < 0.001), as illustrated in Figure 1.
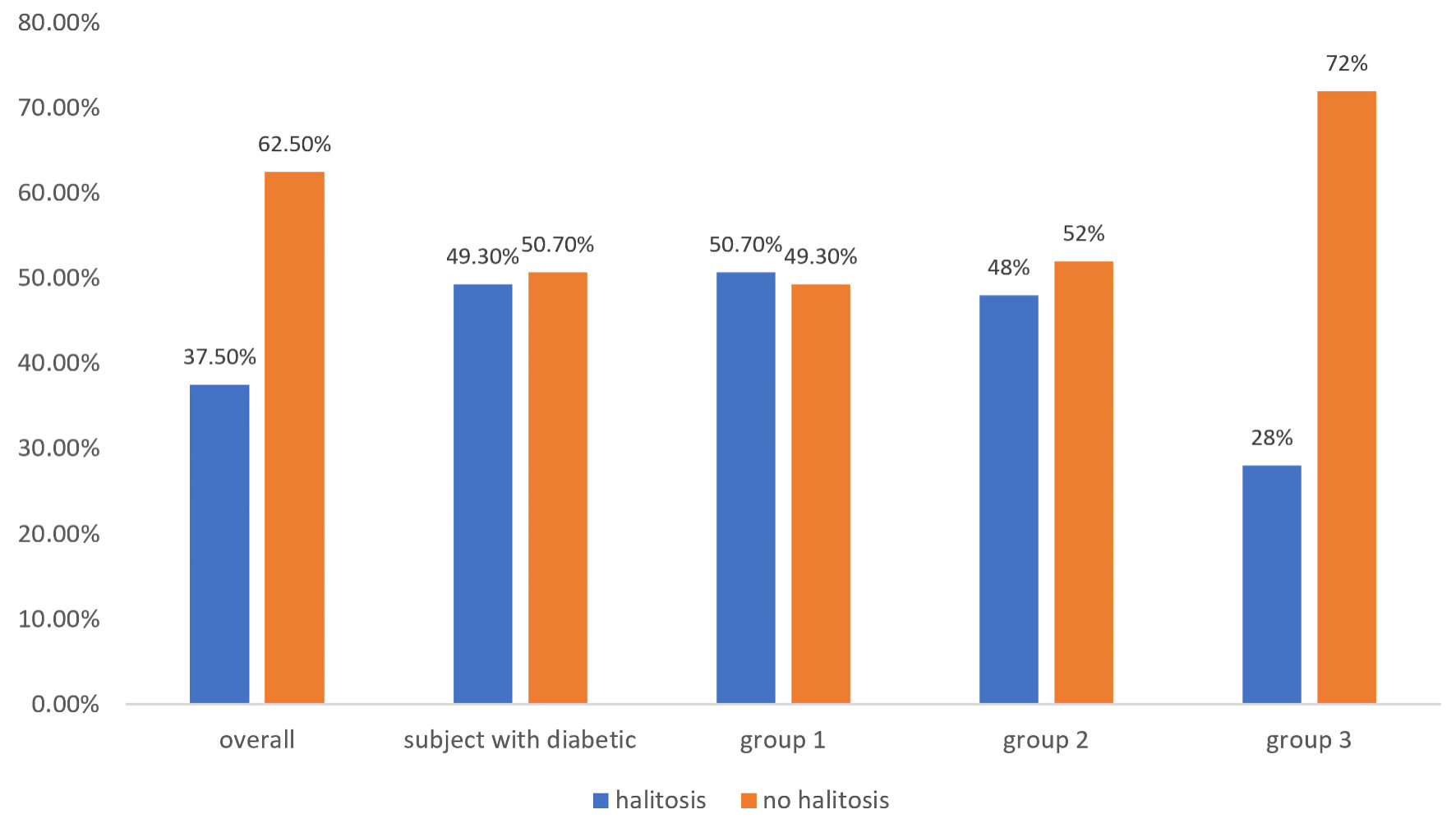 Click for large image | Figure 1. Halitosis prevalence in type 1, type 2, and non-diabetic groups (group 1 = subjects with type 1 DM, group 2 = subjects with type 2 DM, group 3 = non-diabetic subjects). DM: diabetes mellitus. |
Generally, 65.66% of the respondents reported that they follow no specific type of diet. Among the groups, 59.42% of group I, 52.08% of group II, and 73.71% of group III followed no specific diet. Additionally, 34.78%, 42.36%, and 20.86% of groups I, II, and III respectively reported following a low-carb diet (P < 0.001). When comparing patients with type 1 and 2 DM, no significant difference was observed in their diet regimens (low carbs, keto diet, or vegetarian) (P = 0.711) (Table 2).
Click to view | Table 2. Diet Regimen of Participants Among the Three Groups |
When comparing the respondents’ self-reported smelling ability scores, more than 65% reported a score of 8 out of 10 or higher (on a scale from 0 to 10, where 0 indicates anosmia and 10 represents good smelling ability) [19]. A significant difference in self-reported smelling ability was noted between individuals with DM and healthy subjects (P < 0.001) (Fig. 2). However, no significant difference in self-reported smelling ability scores was observed considering diabetes type (group I and group II). Additionally, diabetic subjects in both group I and group II were divided into three subgroups based on the duration of their DM diagnosis (less than 2 years, 2 - 5 years, and more than 5 years). No correlation was found between the duration of DM and self-reported smelling ability (P = 0.858, 0.648 for group I and group II, respectively).
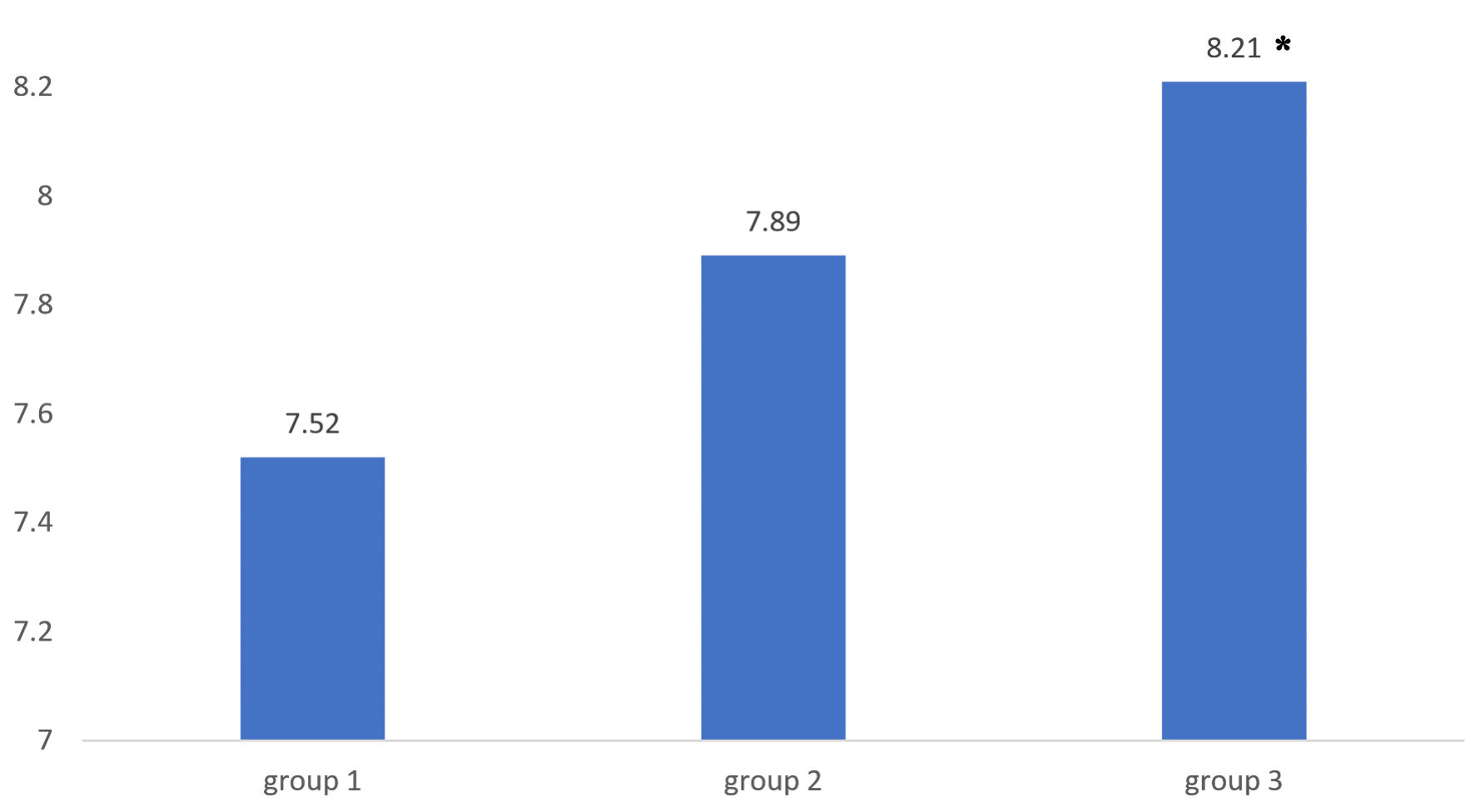 Click for large image | Figure 2. Self-reported smelling ability score among the three groups (group 1 = subjects with type 1 DM, group 2 = subjects with type 2 DM, group 3 = non-diabetic subjects). *Significant difference (P < 0.001). DM: diabetes mellitus. |
Both groups I and II responded similarly when asked if they felt their oral breath smell had changed after being diagnosed with DM (P = 0.899) (Table 3). A significant difference was observed between all groups in terms of the mean reported intensity of halitosis (on a scale from 0 - 10 with 0 indicating no presence of halitosis and 10 as extreme breath malodor) [20] (P = 0.005). However, when specifically comparing type 1 with type 2 diabetes, no statistically significant difference in halitosis intensity was found (P = 0.851) (Fig. 3).
Click to view | Table 3. Prevalence of Halitosis in Patients After Being Diagnosed With DM |
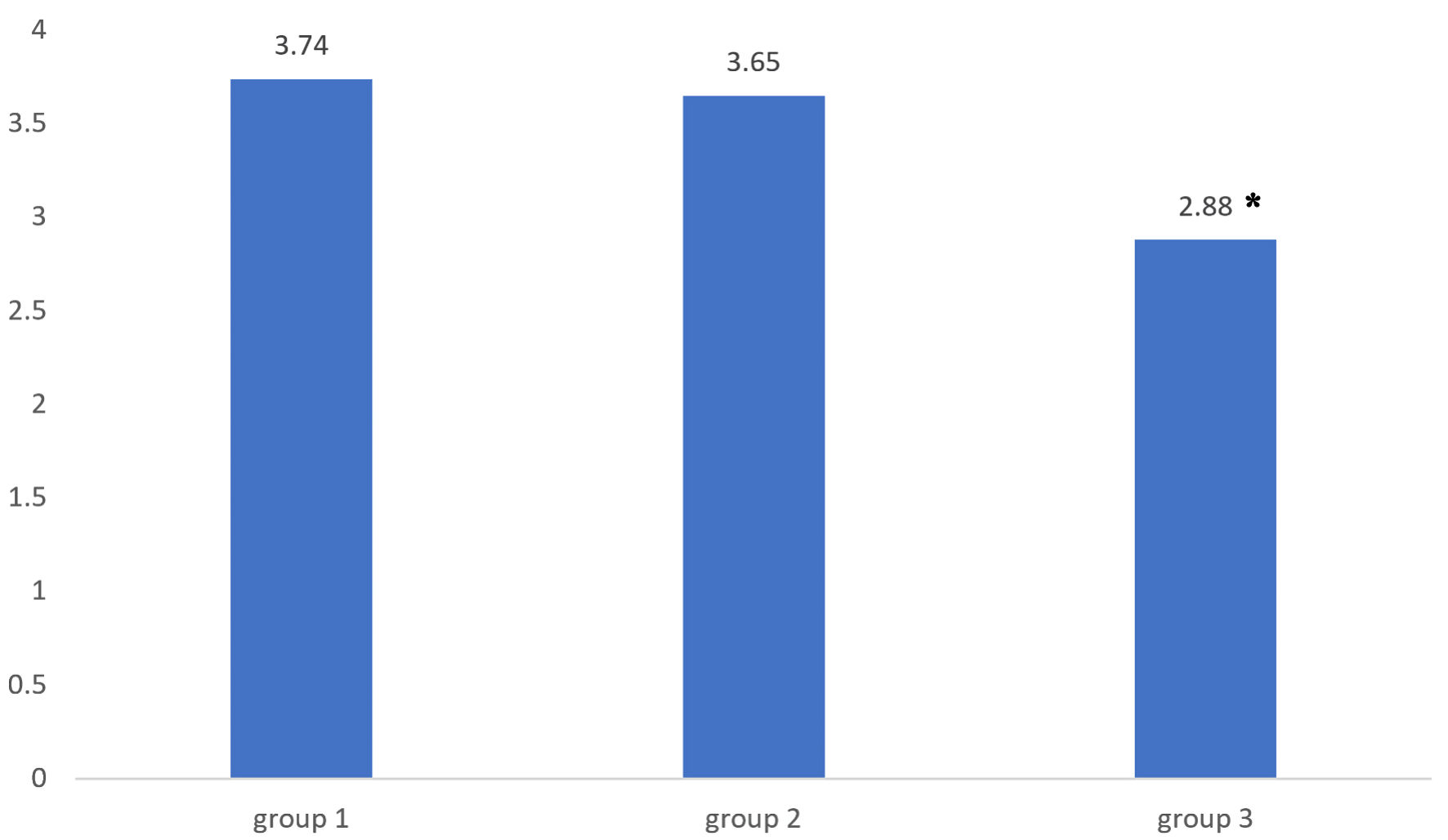 Click for large image | Figure 3. Mean self-reported intensity of halitosis among the three groups (group 1 = subjects with type 1 DM, group 2 = subjects with type 2 DM, group 3 = non-diabetic subjects). *Significant difference (P < 0.005). DM: diabetes mellitus. |
The relationship between diabetes parameters (HbA1c, random blood glucose (RBG)) and self-reported halitosis showed that in group I, 31% reported an increase in oral malodor when RBG levels were elevated, while 19.8% of group II reported the same. However, this difference was not statistically significant. The increase in RBG levels showed no significant effect on halitosis status between groups. (P = 0.151). Similarly, there was no significant correlation between HbA1c levels and the presence (P = 0.983) or intensity (P = 0.654) of the halitosis condition in subjects with DM (Table 4). The mean self-reported halitosis values were 3.71 for type 1 and 3.64 for type 2 diabetes. Additionally, no significant correlation was found between the duration of diabetes and halitosis awareness in patients with type 1 DM (Pearson’s R = 0.162, P = 0.056; Spearman’s correlation = 0.097, P = 0.252) (Table 5). In contrast, a significant time-dependent relationship was observed in the type 2 diabetes group, with a positive correlation, indicating a slight increase in halitosis awareness as the duration of diabetes increased (Pearson’s R = 0.245, P = 0.003; Spearman’s correlation = 0.187, P = 0.023). Out of the 187 subjects with DM who reported presence of halitosis, it is surprising that only 1.7% (11 subjects) were informed about the presence of halitosis by a healthcare provider. In contrast, the majority of subjects (67.4%) recognized the presence of halitosis by themselves.
Click to view | Table 4. Correlation Between HbA1c and Halitosis Score Among Subjects With DM |
Click to view | Table 5. Correlation Between the Duration of DM and Awareness of Halitosis in Group I and Group II |
The study investigated smelling ability, which was believed to be a primary factor influencing halitosis recognition. A statistically significant correlation was observed between smelling ability and the ability to identify halitosis in both group I and group II (P < 0.05). Additionally, the history of COVID-19 infection was recognized as a critical factor affecting olfactory function. Among the participants, 51.3% had contracted COVID-19, and 40.7% reported changes in their smelling ability post-infection. These findings underscore the impact of COVID-19 on olfactory function and its potential influence on halitosis recognition.
| Discussion | ▴Top |
The overall prevalence of halitosis in the study population was 37.5%, which appears higher compared to other studies. Settineri et al reported a lower prevalence of 19.39% among 1,052 patients who reported the presence of halitosis, a difference that can be linked to the younger mean age of the participants [21]. In contrast, Milanesi et al in a self-reported questionnaire of 257 participants, reported a prevalence of 73.5%. This higher prevalence can be attributed to the questionnaire design, where even a single instance of halitosis was considered a positive response, including transient cases like morning breath, which are not often recorded in other surveys [22].
Self-reported halitosis seems to affect a large portion of the diabetic population, with the prevalence reaching 49.3% in this study. In 2011, Al-Zahrani et al conducted a study in Saudi Arabia on 38 patients with type 2 diabetes, similar finding was concluded that 42.1% of the participants have reported presence of halitosis [1]. Shahbaz et al in 2023 examined 214 patients among Pakistani population following up in tertiary hospital, all of whom showed at least three classical signs of DM (polyphagia, polyuria, polydipsia, and general weakness). They reported that 97.6% of the patients with DM were suffering from halitosis. This high prevalence could be linked to the high incidence of generalized periodontitis in their sample, which affected 85.9% of the participants. When comparing diabetic subgroups, a minor difference was noted with halitosis prevalence rates of 50.7% and 48.0% in type 1 and type 2 DM, respectively [23].
A clinical study assessing the presence of VSC in type 1 diabetic patients found that 18% had halitosis, compared to 12% in healthy individuals [24]. The discrepancy with our findings may be due to differences in halitosis assessment methods, age, and diabetes duration. The authors suggested that lower halitosis rates in their study could be attributed to good oral hygiene, controlled diets, and the exclusion of extraoral causes.
The prevalence and intensity of halitosis were higher in both diabetic groups compared to healthy subjects. The high prevalence and intensity among diabetic subjects can be linked to both extraoral and intraoral causes. One prominent extraoral cause in diabetic patients is the increased presence of acetone in the breath due to elevated ketone levels resulting from altered metabolism. Reyes-Reyes et al conducted a study on type 1 diabetic patients, dividing them into three groups: type 1 DM minors (under 15 years), type 1 DM adults (over 15 years) and healthy controls. They measured acetone concentrations in the breath by using quantum cascade laser spectroscopy and found that type 1 diabetic adults showed significantly higher acetone levels compared to healthy subjects, a result that was not observed in minors. The authors suggested that age and the duration of diabetes may play a role in this difference [25]. Li et al evaluated the level of acetone in the breath of 113 type 2 diabetic patients and compared it with 56 healthy controls. Their results showed a significant difference in acetone concentrations, with healthy individuals having an average of 0.72 parts per million by volume (ppmv) compared to 1.75 ppmv in diabetic patients [26].
Another factor contributing to the higher prevalence and intensity of halitosis in subjects with DM is the alteration in the microbiological profile, which increases volatile compounds-producing bacteria. Matsha et al, in a case-control study of 128 subjects comparing subjects with DM, prediabetes and healthy subjects with periodontitis using 16S ribosomal DNA (rDNA) sequencing, found that there is an increase of Fusobacteria and Actinobacteria in individuals with DM and prediabetes compared to non-diabetic subjects [27]. Similarly, Bachtiar et al quantified red complex bacteria in periodontitis patients with or without diabetes and reported that Porphyromonas, Tannerella, and Treponema were significantly more prevalent in the diabetic periodontitis group [28].
Many oral bacteria, especially gram-negative anaerobic species, are found in subgingival biofilm and on the dorsum of the tongue. These gram-negative microorganisms, such as Treponema denticola, Fusobacterium nucleatum, Porphyromonas gingivalis (P. gingivalis), Tannerella forsythensis, Prevotella intermedia, are known to produce oral malodor [29]. Many bacteria, including P. gingivalis, Prevotella intermedia, Fusobacterium nucleatum, Peptostreptococcus micros, Bacteroides forsythus, Campylobacter rectus, Eikenella corrodens and Desulfovibrio species can be located in the periodontal pockets. These are also known to produce VSCs [15, 16]. Further, a previous study reported elevated incidences of Treponema denticola, Prevotella nigrescens, Streptococcus sanguinis, Streptococcus oralis, and Streptococcus intermedius in the supragingival plaque of patients with DM compared to healthy individuals [30]. Collectively, these studies indicated that oral bacteria located in the dorsum of the tongue and in the periodontal pockets are associated with halitosis, and their abundance was significantly correlated with diabetes.
Unlike group I, the duration of diabetes in group II was positively correlated with the length of time individuals were aware of having halitosis. This can be linked to poorer oral hygiene practices due to age differences between the groups and the possibility that group II suffers from more severe periodontal conditions.
To our knowledge, this is the first self-reported survey that assesses halitosis and excludes participants based on their smelling ability. Excluding those with olfactory loss strengthens the study’s reliability by ensuring accurate self-reporting of halitosis.
This study demonstrates a deficiency in the smelling ability of diabetic subjects compared with non-diabetic individuals. Weinstock et al assessed the olfactory accuracy in 111 diabetic subjects using the odorant confusion matrix (OCM); the result showed significantly lower accuracy of olfactory ability among diabetic subjects compared to healthy individuals (67.8% vs. > 80%). This olfactory alteration is likely linked to alterations caused by the diabetic condition [31]. It is important to note that this olfactory impairment may lead to an underestimation of self-reported halitosis prevalence among diabetic patients.
Healthcare providers play a crucial role in diagnosing and informing patients about health conditions, including oral malodor, which can indicate underlying health issues. However, only 4.5% of all individuals reporting oral malodor were informed of their condition by a healthcare provider. Even more surprising, only 1.7% of diabetic subjects were informed about their condition. Bin Mubayrik et al also reported that only 2.3% of 306 female university students suffering from halitosis were informed by their oral health providers [32]. In a broader population, Yu et al reported that only 1.6% of patients were informed by their dentist regarding the presence of halitosis [33]. This low percentage could be attributed to the nature of the disease and the social embarrassment of discussing oral malodor. Additionally, the low reporting rates could be due to a lack of knowledge among dental professionals regarding treatment options. These findings should highlight the need for greater awareness among the dentists’ community to include oral malodor assessment as part of routine examination, especially among diabetic patients. The study has some limitations, including an imbalance in the average age between the groups, which is inherent to the nature of the disease, as type 1 diabetes predominantly affects younger populations. Additionally, the high female-to-male ratio may be attributed to the greater interest and motivation of female participants in the research topic. Another limitation of the study was a recall bias, which can be developed when participants fill out the survey. HbA1c was self-reported by the subjects due to the unavailability of the medical record databases for the participants, which could lead to inaccurate HbA1c values. Thus, the generalization of this study’s conclusion should be taken with caution.
Future clinical research should use more precise methods to assess halitosis in diabetic populations and investigate potential confounding factors, such as periodontal health and lifestyle influences, which may affect the results.
Conclusions
Within the limitations of this study, individuals with DM showed a significant increase in both the prevalence and intensity of halitosis. Both type 1 and type 2 DM demonstrated similar halitosis prevalence, halitosis intensity and smelling ability. HbA1c did not show a direct effect on the halitosis condition in either group. Subjects with DM reported reduced smelling ability compared to healthy individuals, which may contribute to underestimating self-reported halitosis. The combination of reduced smelling ability and insufficient communication from healthcare providers about their condition aggravates the issue for patients with DM.
Acknowledgments
The authors express their sincere appreciation to the Researchers Supporting Project (No. RSP2025R255), King Saud University, Riyadh, Saudi Arabia.
Financial Disclosure
This research was funded by the Researchers Supporting Project (No. RSP2025R255), King Saud University, Riyadh, Saudi Arabia.
Conflict of Interest
The authors declare no conflict of interest related to the manuscript.
Informed Consent
Informed consent was obtained from all participants.
Author Contributions
Conceptualization: MA, HA (Hamad A. Alzoman). Methodology: MA, HA (Hamad A. Alzoman). Validation: MA, SA, HA (Hamad N AlBagieh). Investigation: MA. Resources: HA (Hamad A. Alzoman). Data curation: MA, SA, HA (Hamad A. Alzoman). Writing - original draft preparation: MA, SA, HA (Hamad A. Alzoman). Writing - review and editing: all authors. Supervision: HA (Hamad A. Alzoman). Project administration: MA, HA (Hamad A. Alzoman). Funding acquisition: HA (Hamad A. Alzoman). All authors have read and agreed to the published version of the manuscript
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
DM: diabetes mellitus; IRB: Institutional Review Board; CDRC: College of Dentistry Research Center; S-CVI avg: scale-level content validity index (average); S-CVI UA avg: scale-level content validity index (universal agreement, average); ICC: intraclass correlation coefficient; ANOVA: analysis of variance; HbA1c: hemoglobin A1c; RBG: random blood glucose; VSC: volatile sulfur compounds; ppmv: parts per million by volume; rDNA: ribosomal DNA; OCM: odorant confusion matrix
| References | ▴Top |
- Al-Zahrani MS, Zawawi KH, Austah ON, Al-Ghamdi HS. Self reported halitosis in relation to glycated hemoglobin level in diabetic patients. Open Dent J. 2011;5:154-157.
doi pubmed - Mokeem SA. Halitosis: a review of the etiologic factors and association with systemic conditions and its management. J Contemp Dent Pract. 2014;15(6):806-811.
doi pubmed - Alzoman H, Alssum L, Helmi M, Alsaleh L. Relationship between hormonal changes and self-perceived halitosis in females: a cross-sectional study. Healthcare (Basel). 2022;11(1):43.
doi pubmed - Silva MF, Leite FRM, Ferreira LB, Pola NM, Scannapieco FA, Demarco FF, Nascimento GG. Estimated prevalence of halitosis: a systematic review and meta-regression analysis. Clin Oral Investig. 2018;22(1):47-55.
doi pubmed - Zellmer M, Gahnberg L, Ramberg P. Prevalence of halitosis in elderly living in nursing homes. Int J Dent Hyg. 2016;14(4):295-300.
doi pubmed - Alzoman H. The association between periodontal diseases and halitosis among Saudi patients. Saudi Dent J. 2021;33(1):34-38.
doi pubmed - Roslund K, Lehto M, Pussinen P, Metsala M. Volatile composition of the morning breath. J Breath Res. 2022;16(4):046010.
doi pubmed - Duan X, Chen Z, Xia C, Zhong R, Liu L, Long L. Increased levels of urine volatile organic compounds are associated with diabetes risk and impaired glucose homeostasis. J Clin Endocrinol Metab. 2024;109(2):e531-e542.
doi pubmed - Saasa V, Beukes M, Lemmer Y, Mwakikunga B. Blood ketone bodies and breath acetone analysis and their correlations in type 2 diabetes mellitus. Diagnostics (Basel). 2019;9(4):224.
doi pubmed - Alzahrani HG, AlSarhan MA, Aldohayan A, Bamehriz F, Alzoman HA. Effect of sleeve gastrectomy on the levels of oral volatile sulfur compounds and halitosis-related bacteria. Saudi Dent J. 2024;36(6):940-946.
doi pubmed - Tassopoulos CN, Barnett D, Fraser TR. Breath-acetone and blood-sugar measurements in diabetes. Lancet. 1969;1(7609):1282-1286.
doi pubmed - Cheng S, Poh BR, Tay VWY, Lee PP, Mathur S. The interplay between diabetes Mellitus and soft tissue infections in general surgical patients. BMC Endocr Disord. 2024;24(1):106.
doi pubmed - Berbudi A, Rahmadika N, Tjahjadi AI, Ruslami R. Type 2 Diabetes and its Impact on the Immune System. Curr Diabetes Rev. 2020;16(5):442-449.
doi pubmed - Daniel R, Gokulanathan S, Shanmugasundaram N, Lakshmigandhan M, Kavin T. Diabetes and periodontal disease. J Pharm Bioallied Sci [Internet]. 2012;4(6):280.
doi - Haffajee AD, Socransky SS. Microbial etiological agents of destructive periodontal diseases. Periodontol 2000. 1994;5:78-111.
doi pubmed - Persson S, Edlund MB, Claesson R, Carlsson J. The formation of hydrogen sulfide and methyl mercaptan by oral bacteria. Oral Microbiol Immunol. 1990;5(4):195-201.
doi pubmed - Polit DF, Beck CT. The content validity index: are you sure you know what's being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489-497.
doi pubmed - Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155-163.
doi pubmed - Lotsch J, Hintschich CA, Petridis P, Pade J, Hummel T. Self-ratings of olfactory function and their relation to olfactory test scores. A data science-based analysis in patients with nasal polyposis. Applied Sciences. 2021;11(16):7279.
- Nazir MA, Almas K, Majeed MI. The prevalence of halitosis (oral malodor) and associated factors among dental students and interns, Lahore, Pakistan. Eur J Dent. 2017;11(4):480-485.
doi pubmed - Settineri S, Mento C, Gugliotta SC, Saitta A, Terranova A, Trimarchi G, Mallamace D. Self-reported halitosis and emotional state: impact on oral conditions and treatments. Health Qual Life Outcomes. 2010;8:34.
doi pubmed - Milanesi FC, Kauer B, Wagner TP, Daudt LD, Haas AN. Self-reported halitosis and associated demographic and behavioral factors. Braz Oral Res. 2016;30(1):e71.
doi pubmed - Shahbaz M, Kazmi F, Majeed HA, Manzar S, Qureshi FA, Rashid S. Oral manifestations: a reliable indicator for undiagnosed diabetes mellitus patients. Eur J Dent. 2023;17(3):784-789.
doi pubmed - Iscan TA, Ozsin-Ozler C, Ileri-Keceli T, Guciz-Dogan B, Alikasifoglu A, Uzamis-Tekcicek M. Oral health and halitosis among type 1 diabetic and healthy children. J Breath Res. 2020;14(3):036008.
doi pubmed - Reyes-Reyes A, Horsten RC, Urbach HP, Bhattacharya N. Study of the exhaled acetone in type 1 diabetes using quantum cascade laser spectroscopy. Anal Chem. 2015;87(1):507-512.
doi pubmed - Li W, Liu Y, Lu X, Huang Y, Liu Y, Cheng S, Duan Y. A cross-sectional study of breath acetone based on diabetic metabolic disorders. J Breath Res. 2015;9(1):016005.
doi pubmed - Matsha TE, Prince Y, Davids S, Chikte U, Erasmus RT, Kengne AP, Davison GM. Oral microbiome signatures in diabetes mellitus and periodontal disease. J Dent Res. 2020;99(6):658-665.
doi pubmed - Bachtiar BM, Theodorea CF, Tahapary DL, Astrella C, n/a N, Bachtiar EW. A pilot study of red complex and three genera subgingival microbiome in periodontitis subjects with and without diabetes, evaluated by MinION platform. F1000Res. 2021;10:79.
doi pubmed - Cortelli JR, Barbosa MD, Westphal MA. Halitosis: a review of associated factors and therapeutic approach. Braz Oral Res. 2008;22;(Suppl 1):44-54.
doi pubmed - Hintao J, Teanpaisan R, Chongsuvivatwong V, Ratarasan C, Dahlen G. The microbiological profiles of saliva, supragingival and subgingival plaque and dental caries in adults with and without type 2 diabetes mellitus. Oral Microbiol Immunol. 2007;22(3):175-181.
doi pubmed - Weinstock RS, Wrightt HN, Smitht DU. Olfactory dysfunction in diabetes mellitus olfaction evaluation. Vol. 53. Physiology & Behavior. 1993;53(1):17-21.
- Bin Mubayrik A, Al Hamdan R, Al Hadlaq EM, AlBagieh H, AlAhmed D, Jaddoh H, Demyati M, et al. Self-perception, knowledge, and awareness of halitosis among female university students. Clin Cosmet Investig Dent. 2017;9:45-52.
doi pubmed - Yu WW, Goh R, Cheong E, Guan G, Jin C, Cannon RD, Farella M, et al. Prevalence of halitosis among young adults in Dunedin, New Zealand. Int J Dent Hyg. 2022;20(4):700-707.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.