| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Original Article
Volume 000, Number 000, June 2025, pages 000-000

Dyslipidemia Prevalence and Risk Factors in Al Ain: A Retrospective Cross-Sectional Analysis
Afshan Arshada, f, Ragab Abdulmageda, b, f, Ala Sulimana, c, Marwa Elamina, d, Ahmed Mohameda, e
aBurjeel Royal Hospital, Al Ain, United Arab Emirates
bDubai Academic Health Corporation, Dubai, United Arab Emirates
cMohammed Bin Rashid University of Medicine and Health Sciences, Dubai, United Arab Emirates
dMersey and West Lancashire Teaching Hospitals, Rainhill, UK
eNorth Devon District Hospital, Barnstaple, UK
fCorresponding Author: Afshan Arshad and Ragab Ahmed Abdulmaged, Burjeel Royal Hospital, Al Ain, United Arab Emiratesand
Manuscript submitted February 28, 2025, accepted May 12, 2025, published online June 9, 2025
Short title: Dyslipidemia and Risk Factors in Al Ain
doi: https://doi.org/10.14740/jem1506
| Abstract | ▴Top |
Background: Dyslipidemia, defined by abnormal lipid profiles, is a key modifiable risk factor for cardiovascular diseases (CVDs), contributing significantly to morbidity and mortality globally. Although dyslipidemia prevalence is high in the United Arab Emirates (UAE), data specific to Al Ain City remain limited. The aim of the study was to assess the prevalence of dyslipidemia and its associated risk factors among adults in Al Ain City, UAE, and to inform targeted public health strategies.
Methods: A retrospective, cross-sectional study was conducted at Burjeel Royal Hospital, Al Ain, UAE, utilizing data collected during September - October 2023. Data from 398 adults were analyzed. Participants included outpatient clinic attendees aged ≥ 18 years, with exclusions for pregnant or lactating women and incomplete medical records.
Results: The primary outcome was dyslipidemia prevalence, defined using lipid profile abnormalities. Secondary outcomes included associations with modifiable risk factors such as obesity, hypertension, diabetes, and lifestyle factors. Dyslipidemia prevalence was 66.1%, with males demonstrating higher low-density lipoprotein (LDL) cholesterol levels and females exhibiting higher high-density lipoprotein (HDL) cholesterol levels. Significant risk factors included obesity, hypertension, diabetes, poor dietary habits, and physical inactivity. Older age groups exhibited higher dyslipidemia rates, with notable gender-specific differences in lipid profiles.
Conclusions: The findings reveal a high burden of dyslipidemia in Al Ain, driven by modifiable risk factors. Public health interventions, including lifestyle modifications and routine lipid screening, are urgently needed to mitigate cardiovascular risks. This study establishes a baseline for future regional surveillance and intervention strategies.
Keywords: Lipid disorders; Hypertension; Type 2 diabetes mellitus; Obesity; Body mass index; Internal medicine
| Introduction | ▴Top |
Dyslipidemia, characterized by abnormal lipid levels such as elevated triglycerides, high low-density lipoprotein (LDL) cholesterol, and reduced high-density lipoprotein (HDL) cholesterol (HDL-C), is a significant public health issue due to its role in atherosclerosis and cardiovascular diseases (CVDs) [1]. As CVD remains a leading global cause of morbidity and mortality, addressing dyslipidemia has become central to preventive healthcare strategies [1].
The condition is influenced by both lifestyle and genetic factors. Poor dietary habits, sedentary behavior, smoking, and alcohol consumption are primary contributors [2]. Urbanization and the adoption of Western dietary patterns in the Middle East have further increased its prevalence [2]. Additionally, obesity, hypertension, and diabetes are closely associated with dyslipidemia, reflecting the interplay of metabolic and lifestyle factors [3]. Genetic conditions, including familial hypertriglyceridemia and hypercholesterolemia, also increase susceptibility, often resulting in severe health outcomes [3].
Dyslipidemia is a major contributor to global CVD mortality, accounting for 32% of all deaths in 2019 [4, 5]. In the United Arab Emirates (UAE), CVD accounted for 30% of deaths in 2017, with dyslipidemia being a significant risk factor [6]. Central obesity, strongly linked to dyslipidemia, is highly prevalent in the UAE population, driven by lifestyle factors such as low physical activity and energy-dense diets [7]. Additionally, the high prevalence of metabolic syndrome in the UAE exacerbates the burden of dyslipidemia, with obesity playing a central role in abnormal lipid profiles [8]. Studies indicate that the prevalence of hypercholesterolemia remains persistently high in the UAE, despite advances in medical interventions, highlighting gaps in effective management and prevention strategies [9-11]. Similarly, hypertriglyceridemia, a risk factor for acute pancreatitis, affects a significant portion of the population, further emphasizing the need for public health interventions targeting lipid abnormalities [12]. Moreover, dyslipidemia frequently coexists with type 2 diabetes, which is prevalent in the UAE, compounding the cardiovascular risks and increasing the disease burden [13, 14].
While national-level studies provide valuable insights, there are limited data on city-specific dyslipidemia prevalence in the UAE, particularly in Al Ain. A previous study reported a dyslipidemia prevalence of 62.7%, with higher rates in men (68%) compared to women (54.2%) [15-17]. However, reliance on self-reported data and less rigorous methodologies highlights the need for robust investigations. Comprehensive local data are essential to inform targeted interventions and address unique population characteristics.
This study aimed to bridge this gap by investigating dyslipidemia prevalence and its associated risk factors among adults in Al Ain. It examined modifiable risk factors such as obesity, smoking, diet, and physical activity, alongside genetic determinants like familial hypercholesterolemia. The findings will guide evidence-based public health strategies to mitigate the burden of dyslipidemia and its cardiovascular implications, offering a model for addressing similar challenges in other urban populations.
| Materials and Methods | ▴Top |
A hospital-based, cross-sectional study was conducted at Burjeel Royal Hospital, Al Ain, UAE, from May 2023 to February 2024.
Study population
Adults aged 18 years and older attending the hospital’s outpatient clinics were included. Exclusion criteria were pregnancy or lactation (within 6 months postpartum), incomplete medical records, and secondary causes of dyslipidemia. Out of 408 initially identified participants, 10 with missing data were excluded, leaving a final sample of 398 participants. The sample size was based on a 60% dyslipidemia prevalence estimate in the UAE, a 95% confidence level, and a 5% margin of error, ensuring sufficient power to analyze prevalence and risk factors.
Data collection
Data were sourced from the Integrated Family Health Assessment System (IFHAS), a comprehensive health screening program mandated by the Abu Dhabi Public Health Centre (ADPHC). IFHAS systematically screens patients aged 18 - 75 years to detect and prevent chronic diseases. Its universal and mandatory nature minimizes selection bias and enhances generalizability. Medical records provided demographic variables (age, gender, education, marital status), lifestyle factors (smoking, alcohol consumption, physical activity, diet), and anthropometric measurements (height, weight, body mass index (BMI)). Efforts to reduce selection and information bias included standardized data collection and trained personnel reviews.
Clinical and laboratory assessments
Medical histories were reviewed for hypertension and diabetes, with data derived from routine assessments. Fasting blood samples provided measurements of total cholesterol (TC), LDL cholesterol, HDL-C, triglycerides, and random blood glucose. Dyslipidemia was defined per American College of Cardiology (ACC)/American Heart Association (AHA) guidelines: TC ≥ 5.2 mmol/L, LDL cholesterol ≥ 3.4 mmol/L, HDL-C < 1.0 mmol/L (men) or < 1.3 mmol/L (women), or triglycerides ≥ 1.7 mmol/L. Diabetes was classified as hemoglobin A1c (HbA1c) ≥ 6.5%, and BMI categories included underweight (< 18.5 kg/m2), normal weight (18.5 - 24.9 kg/m2), overweight (25 - 29.9 kg/m2), and obese (≥ 30 kg/m2).
Statistical analysis
Descriptive statistics summarized participant characteristics. Chi-square and t-tests assessed associations between dyslipidemia and risk factors, with logistic regression identifying independent predictors. A P-value < 0.05 was considered statistically significant. Analyses were conducted using Statistical Package for the Social Sciences (SPSS) software version 28.0.
Ethical considerations
Ethical approval was obtained from the Burjeel Institutional Review Board. Informed consent was already part of the IFHAS screening program. All data were retrospectively obtained from existing medical records, adhering to patient privacy and consent protocols.
| Results | ▴Top |
A total of 398 participants were included, with 53.3% male and 46.7% female. The prevalence of abnormal lipid profiles was 66.1%, with males being significantly more affected than females (76.9% vs. 53.8%, P < 0.001). Older age groups, particularly those aged 40 - 49 and ≥ 50 years, had higher dyslipidemia prevalence compared to younger participants (P < 0.001).
BMI was strongly associated with lipid abnormalities, with obese participants showing a markedly higher prevalence (41.4%) compared to those with normal or underweight status (P < 0.001). Smoking was another significant factor, with 25.5% of participants with abnormal lipid profiles being smokers, compared to 11.1% in the normal lipid group (P < 0.001). No significant associations were observed with education level, employment status, or physical activity.
Table 1 summarizes the frequency distribution of key demographic, clinical, and lifestyle characteristics, highlighting significant differences across categories.
 Click to view | Table 1. Frequency Distribution of Demographic, Clinical, and Lifestyle Characteristics in Participants With Normal and Abnormal Lipid Profiles |
Relationship between age and key metabolic parameters
Analysis of the relationship between age and BMI revealed complex patterns. The scatter plot in Figure 1a showed no uniform trend between BMI and age, suggesting that weight changes are influenced by factors beyond chronological aging. While BMI moderately increased with age in some middle-aged clusters, the trend was inconsistent, reflecting variations likely due to lifestyle, genetics, or metabolic changes. Among males, a subtle upward trend in BMI was observed, potentially linked to reduced metabolic rates and activity levels with age. In contrast, females displayed more variability, possibly due to hormonal changes during perimenopause and menopause affecting fat distribution. Younger participants of both genders showed fewer high BMI values, suggesting more active lifestyles and higher metabolic rates, while older participants exhibited wider BMI variability.
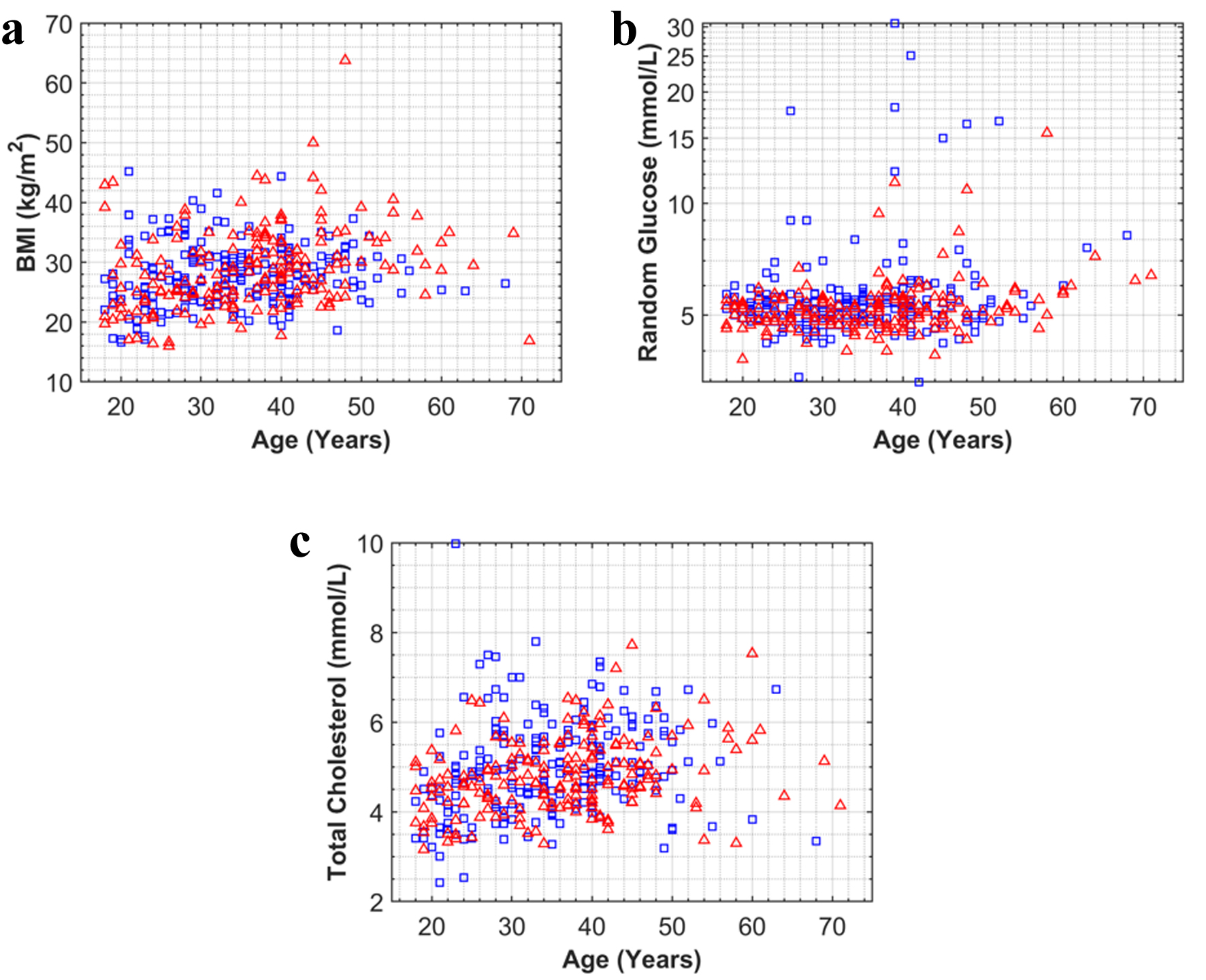 Click for large image | Figure 1. Scatter plots of age (years) versus (a) BMI (kg/m2), (b) random glucose (mmol/L), and (c) total cholesterol (mmol/L) by gender. Males are represented by “□” and females by “Δ”. BMI: body mass index. |
The relationship between age and random blood glucose levels (Fig. 1b) showed no clear trend, indicating that aging alone does not primarily influence glucose regulation. Wide inter-individual variability in glucose levels across all age groups likely reflects differences in dietary habits, physical activity, metabolic conditions, or genetic predispositions. Effective glycemic management may explain the absence of clustering of higher glucose levels in older participants, possibly influenced by a survivorship bias. No significant differences were observed between genders, suggesting potential parity in glucose levels within the cohort, though overlapping distributions highlight the complexity of glucose regulation.
Age and TC levels were also analyzed (Fig. 1c). No significant linear correlation with age was found for either gender, indicating that cholesterol levels are influenced by multiple factors, such as genetics, diet, lifestyle, and comorbid conditions. Male cholesterol levels appeared relatively uniform across age groups, suggesting consistent lipid profiles, potentially due to stable lifestyle factors. In females, a slight increase in cholesterol was observed in post-middle-age groups, possibly due to hormonal changes during menopause, which are known to impact lipid metabolism and cardiovascular risk. Despite these differences, the overall distribution of cholesterol levels between genders showed similarity.
These findings highlight the complexity of metabolic regulation, emphasizing the need for a nuanced understanding of how genetic, environmental, and physiological factors interact to influence BMI, glucose, and cholesterol levels across different age groups and genders.
Correlations among key metabolic and lipid parameters
The correlation heatmap in Figure 2 illustrates relationships among key metabolic and lipid parameters, with correlation coefficients ranging from -1 to 1. Strong positive or negative correlations are closer to 1 or -1, while values near 0 indicate no linear relationship.
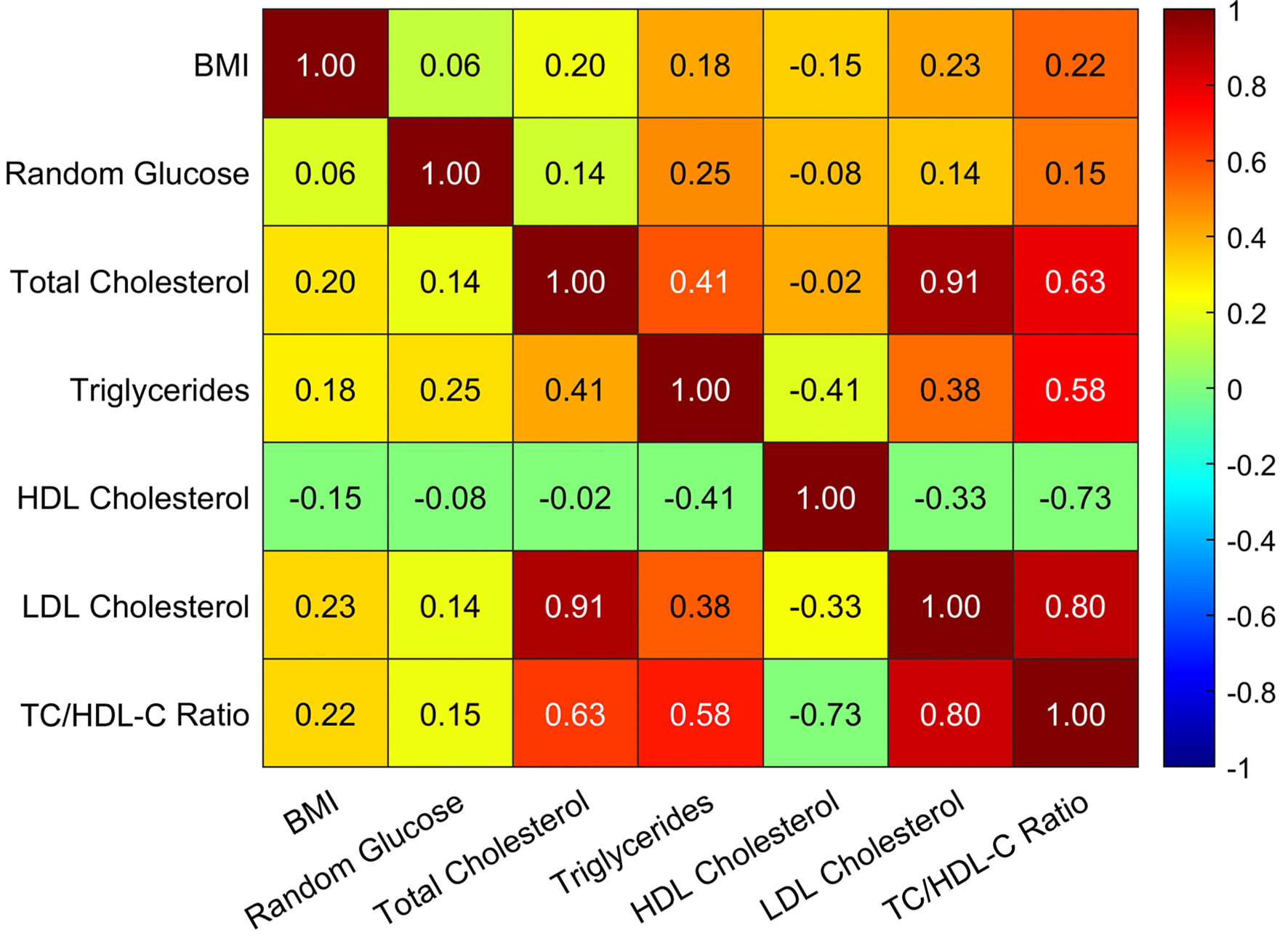 Click for large image | Figure 2. Correlation heatmap illustrating the relationships between key metabolic and lipid parameters (BMI, random blood glucose, TC, triglycerides, HDL cholesterol, LDL cholesterol, and TC to HDL-C ratio), based on the combined data of all participants (both sexes). BMI: body mass index; HDL: high-density lipoprotein; HDL-C: high-density lipoprotein cholesterol; LDL: low-density lipoprotein; TC: total cholesterol. |
Notable correlations include a strong positive association between TC and LDL cholesterol (r = 0.91), highlighting LDL’s significant contribution to TC levels and supporting its role as a target for cardiovascular risk management. The TC to HDL-C ratio, a key cardiovascular risk marker, showed a robust positive correlation with LDL cholesterol (r = 0.80) and a strong negative correlation with HDL-C (r = -0.73), further validating its clinical importance.
BMI demonstrated moderate positive correlations with TC, LDL cholesterol, and the TC to HDL-C ratio, suggesting a link between obesity and dyslipidemia, emphasizing the importance of weight management in mitigating cardiovascular risks. Additionally, HDL-C showed a moderate negative correlation with triglycerides (r = -0.41), consistent with literature indicating their inverse relationship and potential roles in atherosclerosis development.
Impact of physical activity on triglyceride levels
The box plot in Figure 3 illustrates the relationship between exercise frequency and triglyceride levels across four categories: none, little, moderate, and vigorous. Individuals in the “none” category had a wider interquartile range (IQR) and higher median triglyceride levels, indicating greater variability and elevated levels in those without regular physical activity.
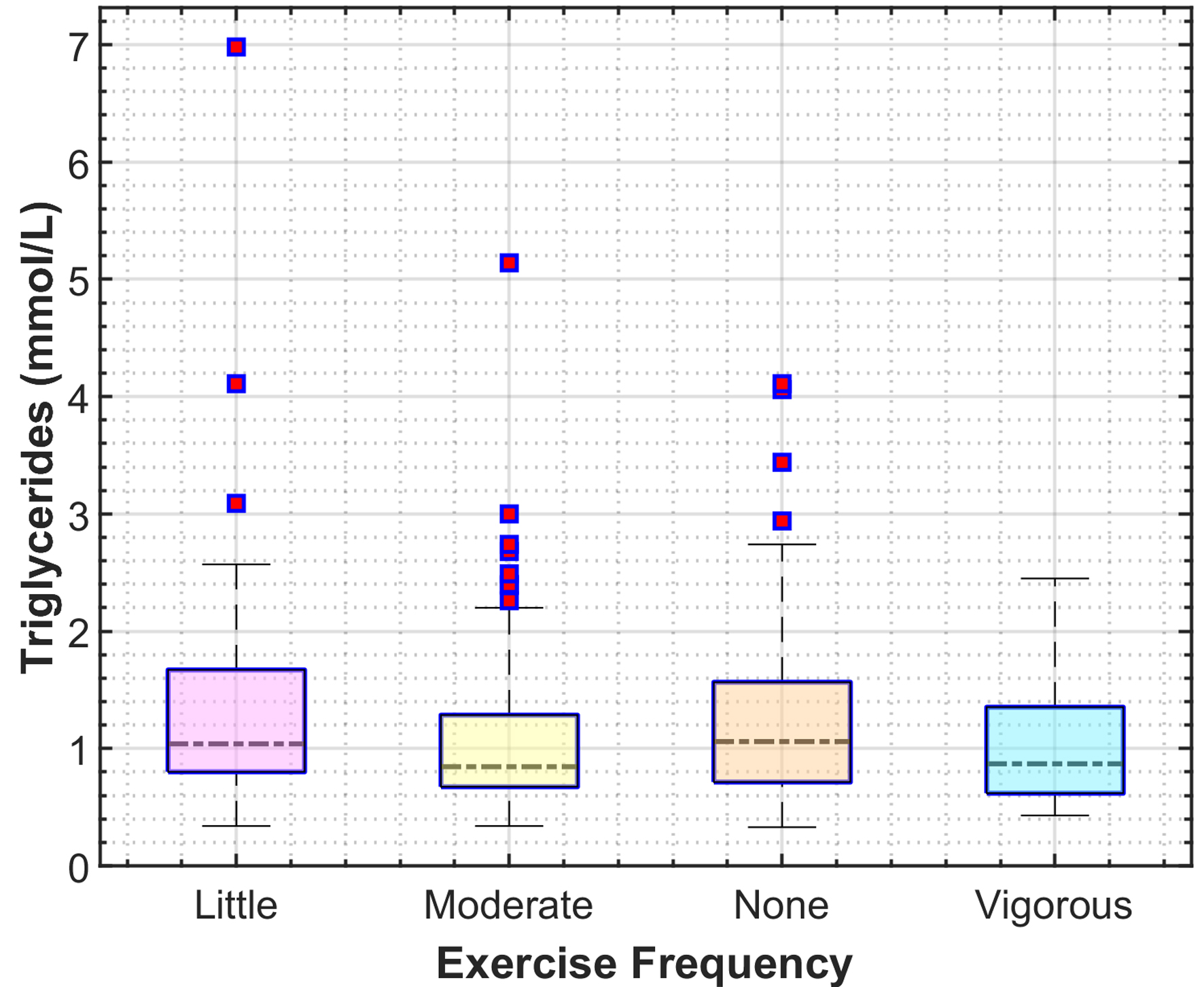 Click for large image | Figure 3. Box plot showing the distribution of triglyceride levels (mmol/L) across four categories of exercise frequency (none, little, moderate, and vigorous), based on the combined data of all participants (both sexes). |
A progressive narrowing of the IQR and a downward shift in median triglyceride levels were observed from the “little” to “vigorous” categories, with the lowest levels in the “vigorous” group. This supports the hypothesis that increased physical activity improves lipid profiles. Additionally, fewer outliers in the more active groups suggest a consistent positive effect of exercise on triglyceride regulation.
While these trends indicate an association between physical activity and lower triglyceride levels, causality cannot be established. Further longitudinal studies are needed to address confounding factors such as diet, genetics, and medication. Nonetheless, these findings align with existing literature advocating physical activity as a non-pharmacological intervention to improve lipid metabolism and reduce cardiovascular risk.
Gender differences in cholesterol levels
The split violin plot in Figure 4 compares cholesterol levels (LDL, HDL, and total) between males and females, with reference lines marking medical cut-off points: 3.4 mmol/L for high LDL, 1.0 mmol/L (males) and 1.3 mmol/L (females) for low HDL, and 5.2 mmol/L for hypercholesterolemia.
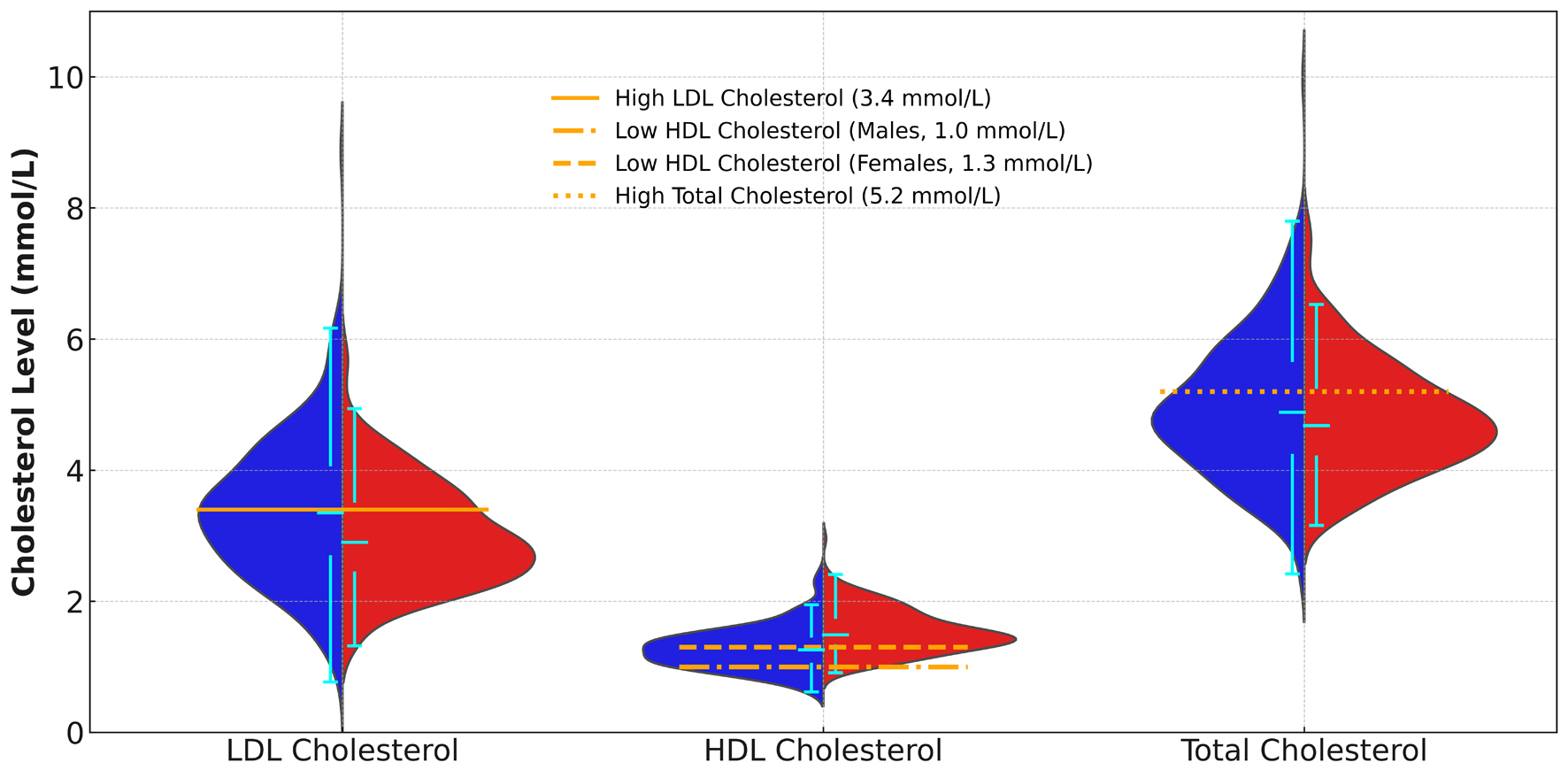 Click for large image | Figure 4. Split violin plot comparing cholesterol levels (LDL, HDL, and total) between male and female participants. Medical cut-off points are indicated for LDL, HDL, and total cholesterol. Male and female data are color-coded using blue and red, respectively. HDL: high-density lipoprotein; LDL: low-density lipoprotein. |
LDL cholesterol levels were widely distributed across both genders, with a substantial proportion exceeding the 3.4 mmol/L threshold, highlighting significant cardiovascular risk. HDL-C showed notable gender differences: most females had levels above 1.3 mmol/L, while many males fell below 1.0 mmol/L, likely due to hormonal influences such as estrogen, which provides cardiovascular protection. These findings align with established research showing higher HDL levels in females.
TC levels also differed by gender, with both males and females frequently exceeding the 5.2 mmol/L cut-off, indicating a high prevalence of hypercholesterolemia and underscoring its public health significance. Elevated TC poses a significant risk for heart disease, requiring targeted management strategies.
These results suggest that biological and hormonal factors play a key role in shaping cholesterol profiles, emphasizing the importance of gender-specific approaches to cardiovascular risk management. Public health initiatives should focus on lifestyle modifications, dietary changes, regular screenings, and medical interventions to address the high prevalence of hypercholesterolemia.
| Discussion | ▴Top |
This study reveals a high prevalence of dyslipidemia (66.1%) among adults in Al Ain City, UAE. Dyslipidemia was significantly associated with modifiable risk factors, particularly obesity, smoking, and older age, with males being disproportionately affected. Conversely, no significant associations were found with education level, employment status, or physical activity. These findings highlight the urgent need for targeted public health interventions to address dyslipidemia and its associated cardiovascular risks.
The study’s strengths include the use of real-world data from a hospital-based screening program, offering comprehensive insights into demographic, clinical, and lifestyle factors. Standardized diagnostic criteria (ACC/AHA guidelines) ensure methodological rigor and comparability with similar studies. However, as a retrospective, single-center study, potential information bias due to incomplete medical records and limited generalizability to the broader UAE population should be acknowledged.
The prevalence reported here aligns with other studies in the UAE and Middle East, reflecting high rates of obesity and diabetes in the region. Similar trends observed in Gulf countries suggest shared risk factors such as dietary patterns and metabolic disorders [18]. Notable gender differences, with males exhibiting higher dyslipidemia prevalence, are consistent with global trends but less frequently emphasized in regional studies. Hormonal and behavioral factors likely contribute to these differences, warranting further investigation [19]. The lack of significant association with physical activity contrasts with international findings highlighting its protective role, suggesting cultural or environmental factors specific to the region [20]. Despite the strong associations with obesity and smoking observed in this study, the absence of a link with physical activity underscores the need for further research into urban Middle Eastern populations.
These findings underscore the necessity for public health initiatives to mitigate dyslipidemia-related risks. Routine lipid profiling, early interventions, and lifestyle modification programs targeting obesity and smoking cessation should be prioritized. Gender-specific strategies are also essential, given the higher prevalence in males. Policymakers should integrate these measures into national screening programs to enhance early detection and reduce the long-term burden of CVD. Limited lipid screening in low- and middle-income regions, including the UAE, delays early intervention and exacerbates dyslipidemia risks [21].
While providing valuable insights, this study leaves several questions unanswered. Future research should explore longitudinal trends in dyslipidemia prevalence and assess the effectiveness of targeted interventions in high-risk groups, particularly males and individuals with obesity. Qualitative studies examining barriers to physical activity and dietary improvements in the local population could further inform public health strategies. Expanding this research across multiple centers in the UAE would enhance generalizability and provide a more comprehensive understanding of dyslipidemia at the national level.
Strengths and limitations of this study
This study is the first to comprehensively evaluate dyslipidemia prevalence and risk factors in Al Ain, providing baseline data for public health strategies.
It uses real-world data from a large hospital-based screening program, ensuring detailed and reliable findings.
Standardized ACC/AHA diagnostic criteria enhance methodological rigor and comparability with other studies.
The retrospective design relying on pre-existing medical records may introduce risks of incomplete or biased data.
Conducting the study at a single tertiary care hospital may limit the generalizability to the broader Al Ain or UAE population.
Conclusion
This study demonstrates a high prevalence of abnormal lipid profiles (66.1%) among adults in Al Ain City, UAE. Significant associations were observed between dyslipidemia and modifiable risk factors, particularly obesity, smoking, and age, with older age groups and those with higher BMI showing an increased prevalence of abnormal lipid profiles. Gender also played a key role, with males being disproportionately affected. However, no significant associations were found with education level, employment status, or physical activity levels. These findings highlight the need for targeted public health interventions focused on lifestyle modification, smoking cessation, routine lipid screening, and early management of cardiovascular risk factors. Given the high burden of dyslipidemia in this population, comprehensive prevention strategies are essential to reduce its impact on cardiovascular health outcomes. Future studies should aim to longitudinally monitor trends in dyslipidemia prevalence and evaluate the efficacy of interventions, particularly in high-risk groups such as males and individuals with obesity.
Acknowledgments
We thank all participants and staff at Burjeel Royal Hospital for their contribution to this study. The guidance and support from the Burjeel Holdings’ Department of Research and Health Innovation were invaluable in the completion of this research.
Financial Disclosure
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of Interest
The authors have no conflict of interest to disclose.
Informed Consent
Participants gave informed consent to participate in the study before taking part.
Author Contributions
AA: conception and design, data analysis and interpretation, manuscript writing, review, and approval. RA: conception and design, manuscript review, and approval. AS: conception and design, data acquisition, manuscript review, and approval. ME and AM: conception and design and data acquisition. RAA and AA are responsible for the overall content as the guarantor.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
ACC: American College of Cardiology; ADPHC: Abu Dhabi Public Health Centre; AHA: American Heart Association; BMI: body mass index; CVD: cardiovascular disease; HbA1c: hemoglobin A1c; HDL: high-density lipoprotein; HDL-C: high-density lipoprotein cholesterol; IFHAS: Integrated Family Health Assessment System; IQR: interquartile range; LDL: low-density lipoprotein; SD: standard deviation; SPSS: Statistical Package for the Social Sciences; TC: total cholesterol; UAE: United Arab Emirates
| References | ▴Top |
- Radaideh G, Al-Dabbas M, Al-Shamali N, et al. Cardiovascular risk factor burden in the United Arab Emirates (UAE): The Africa Middle East (AfME) Cardiovascular Epidemiological (ACE) Study sub-analysis. Int Cardiovasc Forum J. 2017;11:1-5.
doi - Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766-781.
doi pubmed - AMBOSS. Dyslipidemia. AMBOSS. https://next.amboss.com/us/article/4o03XS?q=dyslipidemia#Z0a63013b7ce0e908301d227ca7375bd. Accessed May 24, 2023.
- World Health Organization. The top 10 causes of death. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death. Accessed May 24, 2023.
- Al Sifri SN, Almahmeed W, Azar S, Okkeh O, Bramlage P, Junger C, Halawa I, et al. Results of the Dyslipidemia International Study (DYSIS)-Middle East: clinical perspective on the prevalence and characteristics of lipid abnormalities in the setting of chronic statin treatment. PLoS One. 2014;9(1):e84350.
doi pubmed - Ministry of Health and Prevention in the UAE. Medical experts gathered to highlight relationship between type 2 diabetes and cardiovascular disease. Boehringer Ingelheim. https://www.mea.boehringer-ingelheim.com/press-release/medical-experts-gathered-highlight-relationship-between-type-2-diabetes-and. Published 2022. Accessed May 24, 2023.
- Sulaiman N, Mahmoud I, Hussein A, Elbadawi S, Abusnana S, Zimmet P, Shaw J. Diabetes risk score in the United Arab Emirates: a screening tool for the early detection of type 2 diabetes mellitus. BMJ Open Diabetes Res Care. 2018;6(1):e000489.
doi pubmed - Shin S, Jee H. Prevalence of metabolic syndrome in the Gulf Cooperation Council countries: meta-analysis of cross-sectional studies. J Exerc Rehabil. 2020;16(1):27-35.
doi pubmed - Mahmoud I, Sulaiman N. Dyslipidaemia prevalence and associated risk factors in the United Arab Emirates: a population-based study. BMJ Open. 2019;9(11):e031969.
doi pubmed - Hajat C, Harrison O, Al Siksek Z. Weqaya: a population-wide cardiovascular screening program in Abu Dhabi, United Arab Emirates. Am J Public Health. 2012;102(5):909-914.
doi pubmed - Arafah M, Al-Hinai AT, Al Mahmeed W, Al-Rasadi K, Al Tamimi O, Al Herz S, Al Anazi F, et al. Centralized pan-Middle East Survey on the undertreatment of hypercholesterolemia: results from the CEPHEUS study in Arabian Gulf countries. Angiology. 2014;65(10):919-926.
doi pubmed - de Pretis N, Amodio A, Frulloni L. Hypertriglyceridemic pancreatitis: Epidemiology, pathophysiology and clinical management. United European Gastroenterol J. 2018;6(5):649-655.
doi pubmed - Jelinek HF, Osman WM, Khandoker AH, Khalaf K, Lee S, Almahmeed W, Alsafar HS. Clinical profiles, comorbidities and complications of type 2 diabetes mellitus in patients from United Arab Emirates. BMJ Open Diabetes Res Care. 2017;5(1):e000427.
doi pubmed - Tangvarasittichai S. Oxidative stress, insulin resistance, dyslipidemia and type 2 diabetes mellitus. World J Diabetes. 2015;6(3):456-480.
doi pubmed - Baynouna LM, Revel AD, Nagelkerke NJ, Jaber TM, Omar AO, Ahmed NM, Naziruldeen MK, et al. High prevalence of the cardiovascular risk factors in Al-Ain, United Arab Emirates. An emerging health care priority. Saudi Med J. 2008;29(8):1173-1178.
pubmed - Ali HI, Elmi F, Stojanovska L, Ibrahim N, Cheikh Ismail L, Al Dhaheri AS. Associations of dyslipidemia with dietary intakes, body weight status and sociodemographic factors among adults in the United Arab Emirates. Nutrients. 2022;14(16):3405.
doi pubmed - Mezhal F, Oulhaj A, Abdulle A, AlJunaibi A, Alnaeemi A, Ahmad A, Leinberger-Jabari A, et al. High prevalence of cardiometabolic risk factors amongst young adults in the United Arab Emirates: the UAE Healthy Future Study. BMC Cardiovasc Disord. 2023;23(1):137.
doi pubmed - Alhyas L, McKay A, Balasanthiran A, Majeed A. Prevalences of overweight, obesity, hyperglycaemia, hypertension and dyslipidaemia in the Gulf: systematic review. JRSM Short Rep. 2011;2(7):55.
doi pubmed - Varlamov O, Bethea CL, Roberts CT, Jr. Sex-specific differences in lipid and glucose metabolism. Front Endocrinol (Lausanne). 2014;5:241.
doi pubmed - Yang L, Cao C, Kantor ED, Nguyen LH, Zheng X, Park Y, Giovannucci EL, et al. Trends in sedentary behavior among the US population, 2001-2016. JAMA. 2019;321(16):1587-1597.
doi pubmed - Owolabi M, Miranda JJ, Yaria J, Ovbiagele B. Controlling cardiovascular diseases in low and middle income countries by placing proof in pragmatism. BMJ Glob Health. 2016;1(3):e000105.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.