| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Original Article
Volume 15, Number 3, August 2025, pages 81-90

Impact of the Diabetes Shared Care Program on Glycemic Control in Older Adults With Type 2 Diabetes
Chih-Yen Changa, b, Andrew Y.C. Huangc, Hsiao-Chung Wangd, Shen-Ming Leee, Ching-Sung Hof, g
aDepartment of Nursing, Hsin Sheng Junior College of Medical Care and Management,
Taoyuan, Taiwan, Republic of China
bDepartment of Nursing, Hungkuang University,
Taichung, Taiwan, Republic of China
cSchool of Biological Sciences, University
of California, San Diego, La Jolla, CA 92093, USA
dGraduate Program of
Sustainable Tourism and Recreation Management, National Taichung University of Education,
Taiwan, Republic of China
eDepartment of Statistics, Feng Chia University,
Taichung, Taiwan, Republic of China
fDepartment of Long-Term Care, National
Quemoy University, Jinning Township, Kinmen, Taiwan 89250, Republic of
China
gCorresponding Author: Ching-Sung Ho, Department of Long-Term Care,
National Quemoy University, Jinning Township, Kinmen, Taiwan 89250, Republic of China
Manuscript submitted May 3, 2025, accepted July 8, 2025, published online August 7,
2025
Short title: Glycemic Control in Older Adults With DSCP
doi:
https://doi.org/10.14740/jem1523
| Abstract | ▴Top |
Background: This study aimed to assess the impact of the Diabetes Shared Care Program (DSCP) on glycemic control among elderly patients with type 2 diabetes mellitus (T2DM) over 1 year and identify factors associated with A1C level outcomes.
Methods: A retrospective cohort study was conducted at a regional hospital in central Taiwan from 2016 to 2020. The study included 509 patients aged ≥ 65 years with a confirmed T2DM diagnosis who participated in the program for at least 1 year. A1C levels were analyzed using three thresholds (6.5%, 7%, and 8%), and sociodemographic and health-related factors were examined. Statistical analyses included paired t-tests, the McNemar test, and binary logistic regression models.
Results: After 1 year in the DSCP, the mean A1C level significantly decreased from 7.37 ± 1.30 to 7.11 ± 1.13 (P < 0.001). Glycemic control patterns varied across A1C thresholds, with the most significant improvements observed at the 8% threshold, while improvements were less pronounced at the 6.5% threshold. Abnormal waist circumference was significantly associated with poorer glycemic control, with odds ratios of 2.570 (95% confidence interval (CI): 1.409 - 4.690, P = 0.002) for A1C < 6.5%, 2.360 (95% CI: 1.362 - 4.087, P = 0.002) for A1C < 7%, and 3.169 (95% CI: 1.909 - 5.261, P < 0.001) for A1C < 8%.
Conclusions: The DSCP significantly improved glycemic control in elderly patients with T2DM. Targeted diabetes education interventions should be implemented for older adults at higher risk, particularly those with abnormal waist circumference.
Keywords: T2DM; Elderly; A1C; DSCP
| Introduction | ▴Top |
Diabetes mellitus is a major global health challenge characterized by chronic hyperglycemia and progressive metabolic dysfunction. The World Health Organization (WHO) estimates that over 537 million adults worldwide are living with diabetes, highlighting the urgent need for effective diagnostic and management strategies [1, 2]. In the United States, diabetes is a significant cause of morbidity and mortality, with total expenditures reaching $327 billion in 2017, including $237 billion in direct medical costs and $90 billion in lost productivity [3]. WHO projects that by 2030, diabetes will become one of the world’s leading causes of death, with the mortality rate expected to double between 2005 and 2030 [4]. Diabetes is also a critical public health issue in Taiwan. In 2021, it was the fifth leading cause of death, accounting for 11,450 fatalities [5]. As of 2020, there were approximately 1.74 million patients with diabetes, and the disease accounted for 4.66% of Taiwan’s National Health Insurance (NHI) expenditures, ranking third in total medical costs. The total medical expenditure for diabetes in 2020 amounted to New Taiwan dollars (NT$) 36.4 billion [6].
Aging is a major risk factor for the development and progression of prediabetes and type 2 diabetes mellitus (T2DM). This is largely due to age-related declines in glucose tolerance and increased insulin resistance [7]. T2DM is one of the most prevalent chronic diseases among older adults and is associated with significantly higher morbidity and mortality compared to age-matched non-diabetic individuals [8]. Effective management requires lifelong medication adherence and self-care practices to maintain functional capacity, independence, and quality of life [9]. While pharmacological treatment is essential, self-care behaviors play a crucial role in preventing diabetes-related complications in older adults.
To improve diabetes care and reduce healthcare costs, Taiwan launched the Diabetes Shared Care Program (DSCP) in 2001 [10]. This program is a nationwide, multidisciplinary, and integrated care model aimed at enhancing diabetes management through structured collaboration and standardized clinical protocols. The program brings together primary care physicians, specialists, nurses, and dietitians, all of whom undergo targeted training and certification. Patients are issued diabetes passports to document their clinical progress, and care delivery is centered on the routine monitoring of key health indicators, including blood glucose, glycated hemoglobin (HbA1c), blood pressure, lipid profiles, and renal function. The DSCP places strong emphasis on patient education, self-management, and scheduled follow-ups, all of which are supported by a comprehensive health information system that facilitates appointment scheduling, monitors care quality, and ensures timely clinical interventions [11, 12]. DSCP also offers financial incentives to healthcare providers to encourage continuous follow-up visits and patient engagement in self-care education [13]. Given that diabetes is a complex metabolic disorder requiring ongoing medical supervision, many elderly patients struggle to adopt and sustain lifestyle modifications for effective diabetes management [14]. Therefore, evaluating the effectiveness of DSCP in glycemic control among older adults with diabetes is essential.
Several physical and behavioral factors influence T2DM management outcomes. Obesity, particularly central obesity, is a well-established risk factor for diabetes complications [15]. Waist circumference, a widely used measure of abdominal fat, is a strong predictor of T2DM progression [16]. However, evidence regarding the impact of alcohol consumption on diabetes control remains inconclusive. While some studies suggest that alcohol interferes with self-care behaviors and increases diabetes-related mortality [17], others indicate that moderate alcohol consumption may reduce cardiovascular mortality in diabetic patients [18].
A1C is a well-established marker of long-term glycemic control and is strongly associated with diabetes-related complications and mortality risk [19]. The HbA1c threshold of 6.5% serves as a diagnostic criterion for diabetes and is a key predictor of cardiovascular risk [20, 21]. The 7% threshold is the standard treatment target, balancing glycemic control and complication prevention, while the 8% threshold is often used in elderly or high-risk patients to minimize hypoglycemia-related complications [22-24]. This individualized approach reflects the evolving landscape of diabetes management, where glycemic targets are adjusted based on patient characteristics and clinical risk factors [25]. This stratified approach underscores the evolving understanding of diabetes management, highlighting the intricate relationship between glycemic thresholds, individual patient characteristics, and long-term health outcomes.
Despite the widespread implementation of DSCP, limited research has evaluated its effectiveness among older adults in Taiwan. This study aims to assess the impact of DSCP on glycemic control in elderly patients after 1 year of participation. Additionally, it examines the sociodemographic and health-related factors associated with A1C outcomes, including physical activity, alcohol consumption, body mass index (BMI), and waist circumference.
| Materials and Methods | ▴Top |
Study design
A retrospective cohort study was conducted to achieve the study’s research objectives. The study sample consisted of patients enrolled in the DSCP at a regional hospital in central Taiwan between 2016 and 2020. Clinical data were extracted from medical records after 1 year of program participation.
A total of 509 elderly patients were included in the study. The inclusion criteria required participants to be aged 65 years or older, have a confirmed diagnosis of T2DM, and have participated in the DSCP for at least 1 year. An anonymous data analysis was used to ensure confidentiality, and the study protocol was approved by the Medical Ethics Committee of Jen-Ai Hospital (IRB no. 110-92) on February 18, 2022. The study was conducted in compliance with the ethical standards of the responsible institutional review board and with the principles of the Declaration of Helsinki.
Measurements
The A1C level was selected as the primary outcome variable. A1C was recorded at baseline (upon program enrollment) and subsequently every 3 months. This study compared A1C levels at the end of the first year with baseline values. A1C levels were classified using three clinically relevant thresholds: < 6.5%, < 7%, and < 8%. The independent variables in this study included demographic factors (age, gender, and educational level), health-related behaviors (alcohol consumption (current user vs. none/abstained), cigarette smoking (current user vs. none/abstained), and physical activity (less than three times per week vs. three or more times per week), and anthropometric measurements (BMI and waist circumference). BMI was classified according to the Taiwan Health Promotion Administration’s criteria, with < 24 kg/m2 considered healthy and ≥ 24 kg/m2 classified as abnormal. Waist circumference was defined as abnormal if ≥ 90 cm in men and ≥ 80 cm in women.
Statistical analysis
Descriptive statistics, including frequency analyses, mean values, and standard deviations, were used to summarize A1C levels, sociodemographic characteristics, and health-related factors. To assess the association between A1C levels and related variables, paired t-tests were conducted to compare baseline and 1-year A1C levels, while the McNemar test was used to analyze changes in A1C classification over time. Additionally, binary logistic regression was performed to identify factors associated with A1C outcomes. All statistical analyses were conducted using SPSS version 27.0.
| Results | ▴Top |
Characteristics of the study sample
A total of 509 elderly patients with diabetes were included in this study. Table 1 summarizes the sociodemographic and clinical characteristics of the participants. The study population consisted of 276 females (54.2%) and 233 males (45.8%), with a mean age of 73.54 ± 6.93 years.
 Click to view |
Table 1. Distribution of A1C Level and
Sociodemographic Factors in Elderly Diabetic Patients |
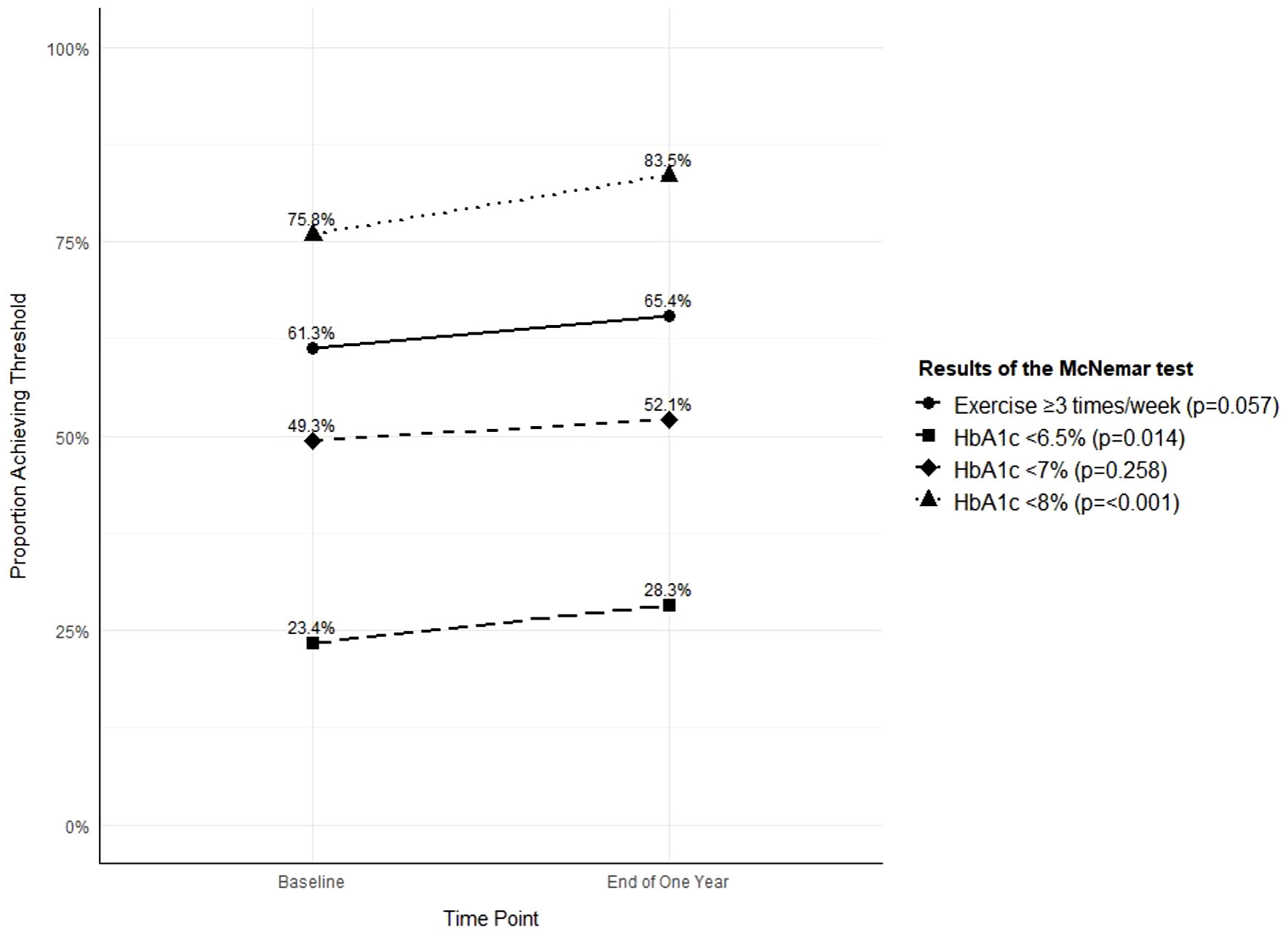
Regarding educational attainment, the majority of participants (39.7%) had 6 or fewer years of education, and 16.7% were illiterate. In contrast, only 12.8% had completed 13 or more years of education. Substance use was relatively low, with 91.7% of participants reporting no alcohol consumption and 90.4% identifying as non-smokers. As for physical activity, 61.3% of participants reported exercising at least three times per week at baseline, increasing to 65.4% at the 1-year follow-up; however, this difference was not statistically significant (P = 0.057) (Fig. 1).
 Click for large image |
Figure 1. Comparison of health threshold achievement before and after DSCP. DSCP: the Diabetes Shared Care Program; HbA1c: glycated hemoglobin. |
BMI and waist circumference assessments indicated potential metabolic risks. Most participants (65.8%) had a BMI of 24 kg/m2 or higher, and 71.7% exhibited abnormal waist circumferences.
Medication adherence was high, with 97.2% taking medication as prescribed and 93.1% adhering to prescribed timing.
Patient characteristics, health-related status, and A1C distribution
At baseline, the mean A1C level was 7.37 ± 1.30. After 1 year of participation in the DSCP, the mean A1C level decreased to 7.11 ± 1.13, a statistically significant reduction (P < 0.001). Differences in A1C level distribution among diabetes patients, as determined by Chi-square (χ2) tests, are presented in Table 2.
Click to view |
Table 2. Distribution of A1C Level at the
Timepoint of Follow-Up After 1 Year in Different Factors |
Gender differences in glycemic control were observed. Males were more likely than females to achieve A1C < 6.5% (32.6% vs. 24.6%, P = 0.029). However, no significant differences were found between genders for A1C < 7% (P = 0.178) or A1C < 8% (P = 0.232).
Educational level was significantly associated with A1C control. Participants with higher education (≥ 13 years) had a greater proportion achieving A1C < 6.5% (43.1%) compared to those with lower education levels (illiterate: 22.4%, P = 0.001). Similar trends were observed for A1C < 7% (P = 0.032), but no significant association was found for A1C < 8% (P = 0.910).
Lifestyle factors also influenced glycemic control. Current alcohol users had significantly better glycemic control at the A1C < 7% threshold (73.8% vs. 50.1%, P = 0.002) but not at other thresholds. Smoking status was not significantly associated with A1C control at any threshold.
BMI and waist circumference played a crucial role in glycemic control. Participants with BMI < 24 kg/m2 had significantly better A1C control at all thresholds (P < 0.05), with 39.1% achieving A1C < 6.5%, compared to 22.7% among those with BMI ≥ 24 (P < 0.001). Similarly, normal waist circumference was strongly associated with better glycemic control across all A1C thresholds (P < 0.01).
Physical activity also influenced glycemic control. Engaging in exercise ≥ 3 times per week was significantly associated with better A1C control at the A1C < 6.5% (P = 0.026) and A1C < 8% (P = 0.002) thresholds.
Regarding medication adherence, no significant differences in glycemic control were observed between participants who adhered to their prescribed medication or medication timing and those who did not.
These findings suggest that educational level, BMI, waist circumference, and exercise frequency play crucial roles in glycemic control after 1 year of participation in the DSCP.
McNemar test for A1C levels
A1C levels at baseline and at the timepoint of follow-up after 1 year were compared using three threshold criteria (6.5%, 7%, and 8%). The McNemar test was performed to assess changes in glycemic control over time (Fig. 1).
At the 6.5% threshold, 69.7% (83/119) of participants with baseline A1C < 6.5% maintained good glycemic control at 1 year, while 30.3% (36/119) experienced deterioration to ≥ 6.5%. Among participants with baseline A1C ≥ 6.5%, 15.6% (61/390) improved to < 6.5%, while 84.4% (329/390) remained at ≥ 6.5%. By the end of 1 year, 28.3% (144/509) of participants had A1C < 6.5%, while 71.7% (365/509) had A1C ≥ 6.5%. McNemar test indicated a statistically significant improvement in glycemic control at this threshold (P = 0.014).
At the 7% threshold, 76.5% (192/251) of participants with baseline A1C < 7% maintained this level at 1 year, while 23.5% (59/251) increased to ≥ 7%. Among those with baseline A1C ≥ 7%, 28.3% (73/258) improved to < 7%, while 71.7% (185/258) remained at ≥ 7%. At 1 year, 52.1% (265/509) of participants had A1C < 7%, compared to 47.9% (244/509) with A1C ≥ 7%. The McNemar test showed no significant difference between baseline and 1-year measurements at this threshold (P = 0.258).
At the 8% threshold, 93.3% (360/386) of participants with baseline A1C < 8% maintained this level at 1 year, while only 6.7% (26/386) increased to ≥ 8%. Among those with baseline A1C ≥ 8%, 52.8% (65/123) improved to < 8%, while 47.2% (58/123) remained at ≥ 8%. By the end of 1 year, 83.5% (425/509) of participants had A1C < 8%, whereas 16.5% (84/509) had A1C ≥ 8%. The McNemar test demonstrated a highly significant improvement at this threshold (P < 0.001).
These findings indicate that glycemic control patterns varied significantly across different A1C thresholds. The most substantial improvements were observed at the 8% threshold, while moderate but significant changes occurred at the 6.5% threshold.
Binary logistic regressions
Table 3 presents the results of binary logistic regression analyses identifying factors associated with glycemic control at different A1C thresholds (8%, 7%, and 6.5%) at the timepoint of follow-up after 1 year.
Click to view |
Table 3. Logistic Regression Analysis of A1C
Levels at the Timepoint of Follow-Up After 1 Year Across Different
Thresholds |
For A1C < 6.5%, abnormal waist circumference was significantly associated with poorer glycemic control (odds ratio (OR) = 2.570, 95% confidence interval (CI): 1.409 - 4.690, P = 0.002). Baseline abnormal A1C levels showed the strongest association at this threshold (OR = 11.836, 95% CI: 7.718 - 19.517, P < 0.001). Gender, education level, BMI, alcohol consumption, and exercise frequency were not significantly associated with glycemic control at this level. The model explained 37.3% of the variance (R2 = 0.373).
For A1C < 7%, abnormal waist circumference was a significant predictor of poorer glycemic control (OR = 2.360, 95% CI: 1.362 - 4.087, P = 0.002). Baseline A1C levels demonstrated an even stronger association (OR = 8.150, 95% CI: 5.378 - 12.351, P < 0.001). Education level and BMI were not significantly associated. The model explained 34.8% of the variance (R2 = 0.348).
Across all three A1C thresholds, abnormal baseline A1C levels consistently exhibited the strongest association with poor glycemic control, with increasing ORs as the threshold became more stringent (from OR = 5.620 at < 8% to OR = 11.836 at < 6.5%). Similarly, abnormal waist circumference was consistently associated with poorer glycemic control, though its effect size decreased as the threshold became more stringent.
For A1C <8%, abnormal waist circumference was significantly associated with poorer glycemic control (OR = 3.169, 95% CI: 1.909 - 5.261, P < 0.001). Exercising fewer than three times per week showed a marginally significant association with poorer glycemic control compared to exercising ≥ 3 times per week (OR = 1.107, 95% CI: 0.742 - 1.653, P = 0.049). Baseline abnormal A1C levels strongly predicted continued poor glycemic control at 1 year (OR = 5.620, 95% CI: 3.447 - 9.161, P < 0.001). BMI ≥ 24 kg/m2 was not significantly associated (OR = 0.954, 95% CI: 0.599 - 1.520, P = 0.843). The model explained 21.3% of the variance (R2 = 0.213).
| Discussion | ▴Top |
This study evaluated the effectiveness of the DSCP in improving glycemic control among older adults with diabetes. Comparisons with previous studies on diabetes self-care education programs have yielded inconsistent findings. While Gagliardino et al reported improved A1C levels following a 1-year education program [26], another study found no significant change after a similar intervention [27]. Our results demonstrate that elderly diabetic patients in Taiwan experienced a significant reduction in HA1c levels after 1 year in the DSCP (7.37±1.30% vs. 7.11±1.13%, P < 0.001). However, A1C changes varied across different glycemic thresholds. The greatest improvement was observed at the 8% threshold, where 52.8% of participants with baseline A1C ≥ 8% achieved A1C < 8% at follow-up (P < 0.001). This success rate aligns with findings from the ACCORD trial, which reported that 50-55% of patients with baseline A1C ≥ 8% achieved values below this threshold after intensive intervention [28]. Notably, 93.3% of participants who attained A1C < 8% maintained this level, suggesting that preventing severe hyperglycemia is more feasible than sustaining stricter glycemic targets. This finding aligns with observations by Tricco et al (2018) in a systematic review of diabetes management strategies [29].
At the 7% threshold, which aligns with targets recommended by multiple diabetes associations [30], we observed no statistically significant difference between baseline and 1-year measurements (P = 0.258). Although 28.3% of participants with baseline A1C ≥ 7% improved to < 7%, a notable 23.5% of those with initially good control deteriorated to ≥ 7%, resulting in only a modest net improvement (52.1% vs. 47.9%). This improvement falls short of the 35-40% success rate reported by Blonde et al (2018) following the initiation of new therapies [31]. These discrepancies may reflect the challenges of maintaining glycemic control in real-world settings, where adherence and healthcare access differ from clinical trial conditions.
For the most stringent 6.5% threshold, we observed a statistically significant improvement (P = 0.014), though the pattern differed from that seen with the 8% threshold. While 15.6% of participants with baseline A1C ≥ 6.5% improved to < 6.5%, a concerning 30.3% of those with initially good control deteriorated to ≥ 6.5%. This trend mirrors findings from the VADT study, which highlighted the difficulty of maintaining tight glycemic control over time [32]. Similarly, Khunti et al (2018) reported that only 13-18% of patients sustain A1C < 6.5% over multiple years [33].
The declining success rates with increasingly stringent targets (52.8% at < 8%, 28.3% at < 7%, and 15.6% at < 6.5%) emphasize the progressive difficulty of achieving tight glycemic control. This phenomenon, termed “therapeutic inertia”, reflects both physiological limitations and healthcare system challenges [34]. Notably, glycemic deterioration was more common at the 6.5% threshold (30.3%) than at the 7% (23.5%) or 8% (6.7%) thresholds, suggesting that maintaining very tight control requires more intensive monitoring and intervention, as noted by Davies et al (2022) [35].
These findings have important clinical implications. First, setting individualized glycemic targets based on patient characteristics and baseline control may be more effective than applying uniform thresholds. This approach aligns with the personalized recommendations of the American Diabetes Association and the European Association for the Study of Diabetes [36]. Second, the higher success rate at the 8% threshold suggests that prioritizing patients with the poorest glycemic control could provide the greatest population-level benefits. This observation is consistent with findings by Vijan et al (2014) [37]. Finally, the significant deterioration rate at the 6.5% threshold underscores the need for vigilant monitoring and more aggressive interventions for patients who initially achieve tight glycemic control.
Our logistic regression analysis revealed several important associations between various factors and glycemic control across different A1C thresholds (< 8%, < 7%, and < 6.5%). The most consistent and powerful predictor across all thresholds was the baseline A1C level. Patients with abnormal baseline A1C levels had significantly higher odds of maintaining elevated A1C levels at the timepoint of follow-up after 1 year, with ORs increasing progressively as the threshold became more stringent (OR = 5.620 at < 8%, OR = 8.150 at < 7%, and OR = 11.836 at < 6.5%; all P < 0.001). This strong association underscores the importance of early intervention and the challenges in achieving glycemic targets for patients who begin with poor glycemic control. These findings underscore the importance of early intervention, as previously demonstrated by Lachin et al (2014) [38], and the recommendations from the American Diabetes Association (2023) [30].
Waist circumference also emerged as a significant predictor across all thresholds. Patients with abnormal waist circumference had 2.36 - 3.62 times higher odds of elevated A1C levels at 1 year (all P ≤ 0.002). This aligns with established research linking central adiposity to insulin resistance and poor glycemic outcomes, independent of overall BMI. Similar findings were reported by Kodama et al (2012) in a meta-analysis of 15 prospective studies [39]. Interestingly, BMI itself was not significantly associated with A1C outcomes at any threshold (P > 0.05), suggesting that fat distribution, rather than total body mass, may be a more relevant metabolic risk factor [40]. This discrepancy between BMI and waist circumference as predictors of glycemic control has also been noted by Janiszewski et al (2008), who found that central adiposity was a stronger predictor of insulin resistance than BMI [41].
Exercise frequency showed a marginally significant association only at the < 8% threshold (P = 0.049), with patients exercising less than three times per week having slightly higher odds of elevated A1C levels. This association was not observed at the more stringent thresholds, suggesting that while physical activity may help patients achieve modest glycemic targets, additional interventions may be necessary for more intensive glycemic control. These results partially contrast with the findings of Colberg et al (2016), who reported more substantial benefits of regular exercise across all levels of glycemic control [42], suggesting that exercise intensity and type, not captured in our model, may play a role.
Regarding sociodemographic factors, neither gender nor education level showed consistent significant associations with glycemic outcomes, though there was a trend toward better outcomes in more educated patients at the < 6.5% threshold. This trend is consistent with findings from Walker et al (2020), who reported that higher education levels were associated with better diabetes self-management and glycemic control [43]. Similarly, alcohol consumption did not demonstrate a significant impact on glycemic control at the < 6.5% threshold (P = 0.266), which contrasts with some studies suggesting moderate alcohol consumption may improve insulin sensitivity [44]. Some studies have demonstrated that male diabetic patients exhibit better self-care practices than females [45, 46]. However, other research has indicated that gender does not result in differential levels of self-care [47]. Our study reveals that the normal rate distribution for the A1C level at the end of 1 year does not exhibit any significant gender difference. Further investigation is necessary to determine the influence of gender on diabetes disease control.
This study evaluates changes in HbA1c as the primary outcome before and after participation in the DSCP. Explanatory variables include data collected at the 1-year follow-up, as certain factors, such as gender and educational level, are fixed and not expected to change over time. Health-related behaviors and process indicators (e.g., medication adherence, substance use) were assessed only at the 1-year follow-up, with the aim of determining whether participants were adhering to appropriate diabetes self-care practices after completing 1 year in the DSCP.
It is well established that medication adherence plays a critical role in the regulation of A1C [48]. In our study, over 90% of elderly patients with diabetes reported taking their medication as prescribed, including proper timing and adherence. However, medication-related factors were not significantly associated with differences in the distribution of A1C thresholds. The impact of medication adherence on glycemic control warrants further investigation.
Our study possesses several strengths, including its retrospective design and long-term follow-up period, which facilitated the evaluation of the program’s effect on the T2DM population and the longitudinal relationship between health behaviors and A1C levels. Our study examines glycemic control across multiple clinically relevant thresholds, providing a nuanced view of diabetes management outcomes.
However, this study has certain limitations. The study sample was derived from a single metropolitan-regional hospital in central Taiwan; therefore, the findings may not be generalizable to all older diabetic patients. These results should be interpreted in the context of certain limitations, including the lack of information about specific interventions, medication adherence, and lifestyle modifications that might have influenced glycemic trajectories [49]. The independent variables were retrieved at the end of 1 year, necessitating further exploration of the actual effects of factors relating to the A1C level. Future research should consider examining the relationship between patterns of obesity, such as waist circumference and BMI, or alcohol consumption, and changes in A1C levels. Future studies could expand on this work by incorporating longitudinal data and exploring additional covariates to refine these predictive models.
Conclusions
The DSCP effectively lowers A1C levels in elderly patients with diabetes. Given the positive correlation between education level and self-care behaviors in this population, health authorities should implement additional diabetes education interventions for less-educated patients.
Compared to BMI, waist circumference may serve as a more reliable predictor of diabetes control outcomes. Older adults with diabetes face a higher risk of chronic microvascular and macrovascular complications. Additionally, they may have fewer resources for managing their condition than younger individuals, highlighting the need for enhanced self-management support.
The identified critical thresholds warrant attention in clinical practice and serve as a foundation for further research aimed at optimizing patient outcomes through tailored interventions.
Acknowledgments
None to declare.
Financial Disclosure
No funding was received for this study.
Conflict of Interest
The authors declare that they have no competing interest.
Informed Consent
Not applicable
Author Contributions
Chih-Yen Chang: writing - original draft preparation, data curation, software, validation. Andrew Y.C. Huang: investigation, writing - reviewing and editing. Hsiao-Chung Wang: data curation, software, validation. Shen-Ming Lee: writing - reviewing and editing. Ching-Sung Ho: conceptualization, methodology, and visualization. All authors contributed to the preparation of the final manuscript.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- International Diabetes Federation. IDF Diabetes Atlas. 10th ed. 2023.
- World Health Organization. Global Report on Diabetes. WHO Technical Report Series. 2023.
- American Diabetes Association. Economic costs of diabetes in the U.S.
in 2017. Diabetes Care. 2018;41(5):917-928.
doi pubmed - Das H, Naik B, Behera H. Classification of diabetes mellitus disease
(DMD): a data mining (DM) approach. In: Progress in Computing, Analytics, and Networking.
Springer; 2018:539-549.
doi - Ministry of Health and Welfare. The top 10 causes of death in Taiwan in 2021. Accessed November 24, 2023. https://www.mohw.gov.tw/cp-16-70314-1.html.
- National Health Insurance Administration. The top 20 diseases of the National Health Insurance program expenditures. Accessed November 24, 2023. https://www.nhi.gov.tw/Content_List.aspx?n=D529CAC4D8F8E77B&topn=23C660CAACAA159D.
- Chang AM, Halter JB. Aging and insulin secretion.
Am J Physiol Endocrinol Metab. 2003;284(1):E7-12.
doi pubmed - Abi Khalil C, Roussel R, Mohammedi K, Danchin N, Marre M.
Cause-specific mortality in diabetes: recent changes in trend mortality.
Eur J Prev Cardiol. 2012;19(3):374-381.
doi pubmed - Francisco PM, Belon AP, Barros MB, Carandina L, Alves MC, Goldbaum M,
Cesar CL. [Self-reported diabetes in the elderly: prevalence, associated factors, and control
practices]. Cad Saude Publica. 2010;26(1):175-184.
doi pubmed - Liang YW, Chang HF, Lin YH. Effects of health-information-based
diabetes shared care program participation on preventable hospitalizations in Taiwan. BMC Health
Serv Res. 2019;19(1):890.
doi pubmed - Chiou ST, Lin HD, Yu NC, Hseuh HK, Lin LH, Lin LT, Chen TJ, et al. An
initial assessment of the feasibility and effectiveness of implementing diabetes shared care
system in Taiwan—some experiences from I-Lan County. Diabetes Res Clin Pract.
2001;54(Suppl 1):S67-73.
doi pubmed - Chen HS. The effects of diabetes share care program in southern
Taiwan. J Chin Med Assoc. 2011;74(7):283-284.
doi pubmed - Lee TT, Cheng SH, Chen CC, Lai MS. A pay-for-performance program for
diabetes care in Taiwan: a preliminary assessment. Am J Manag Care.
2010;16(1):65-69.
pubmed - American Diabetes A. Standards of medical care for patients with
diabetes mellitus. Diabetes Care. 2003;26(Suppl 1):S33-50.
doi pubmed - Gray N, Picone G, Sloan F, Yashkin A. Relation between BMI and
diabetes mellitus and its complications among US older adults. South Med J.
2015;108(1):29-36.
doi pubmed - Siren R, Eriksson JG, Vanhanen H. Waist circumference a good
indicator of future risk for type 2 diabetes and cardiovascular disease. BMC Public Health.
2012;12:631.
doi pubmed - Engler PA, Ramsey SE, Smith RJ. Alcohol use of diabetes patients: the
need for assessment and intervention. Acta Diabetol. 2013;50(2):93-99.
doi pubmed - Valmadrid CT, Klein R, Moss SE, Klein BE, Cruickshanks KJ. Alcohol
intake and the risk of coronary heart disease mortality in persons with older-onset diabetes
mellitus. JAMA. 1999;282(3):239-246.
doi pubmed - Khaw KT, Wareham N, Bingham S, Luben R, Welch A, Day N. Association
of hemoglobin A1c with cardiovascular disease and mortality in adults: the European prospective
investigation into cancer in Norfolk. Ann Intern Med. 2004;141(6):413-420.
doi pubmed - Selvin E, Steffes MW, Zhu H, Matsushita K, Wagenknecht L, Pankow J,
Coresh J, et al. Glycated hemoglobin, diabetes, and cardiovascular risk in nondiabetic adults.
N Engl J Med. 2010;362(9):800-811.
doi pubmed - American Diabetes Association. Standards of Medical Care in Diabetes-2024. Diabetes Care. 2024;47(Suppl 1):S1-S328.
- Ismail-Beigi F, Craven T, Banerji MA, Basile J, Calles J, Cohen RM,
Cuddihy R, et al. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in
type 2 diabetes: an analysis of the ACCORD randomised trial. Lancet.
2010;376(9739):419-430.
doi pubmed - Action to Control Cardiovascular Risk in Diabetes Study Group,
Gerstein HC, Miller ME, Byington RP, Goff DC, Jr., Bigger JT, Buse JB, et al. Effects of
intensive glucose lowering in type 2 diabetes. N Engl J Med.
2008;358(24):2545-2559.
doi pubmed - Freeman J. Management of hypoglycemia in older adults with type 2
diabetes. Postgrad Med. 2019;131(4):241-250.
doi pubmed - Huang ES, Liu JY, Moffet HH, John PM, Karter AJ. Glycemic control,
complications, and death in older diabetic patients: the diabetes and aging study. Diabetes
Care. 2011;34(6):1329-1336.
doi pubmed - Gagliardino JJ, Etchegoyen G, PEDNID-LA Research Group. A model
educational program for people with type 2 diabetes: a cooperative Latin American implementation
study (PEDNID-LA). Diabetes Care. 2001;24(6):1001-1007.
doi pubmed - Gabbay RA, Lendel I, Saleem TM, Shaeffer G, Adelman AM, Mauger DT,
Collins M, et al. Nurse case management improves blood pressure, emotional distress and diabetes
complication screening. Diabetes Res Clin Pract. 2006;71(1):28-35.
doi pubmed - ACCORD Study Group, Gerstein HC, Miller ME, Genuth S, Ismail-Beigi F,
Buse JB, Goff DC, Jr., et al. Long-term effects of intensive glucose lowering on cardiovascular
outcomes. N Engl J Med. 2011;364(9):818-828.
doi pubmed - Tricco AC, Ivers NM, Grimshaw JM, Moher D, Turner L, Galipeau J,
Halperin I, et al. Effectiveness of quality improvement strategies on the management of
diabetes: a systematic review and meta-analysis. Lancet. 2012;379(9833):2252-2261.
doi pubmed - ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D,
Collins BS, et al. 2. Classification and diagnosis of diabetes: standards of care in
diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S19-S40.
doi pubmed - Blonde L, Khunti K, Harris SB, Meizinger C, Skolnik NS.
Interpretation and impact of real-world clinical data for the practicing clinician. Adv Ther.
2018;35(11):1763-1774.
doi pubmed - Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reaven PD,
Zieve FJ, et al. Glucose control and vascular complications in veterans with type 2 diabetes.
N Engl J Med. 2009;360(2):129-139.
doi pubmed - Khunti K, Gomes MB, Pocock S, Shestakova MV, Pintat S, Fenici P,
Hammar N, et al. Therapeutic inertia in the treatment of hyperglycaemia in patients with type 2
diabetes: A systematic review. Diabetes Obes Metab. 2018;20(2):427-437.
doi pubmed - McCoy RG, O'Connor PJ. Overcoming therapeutic inertia in type 2
diabetes care-timing, context, and appropriateness of treatment intensification. JAMA Netw Open.
2021;4(10):e2130926.
doi pubmed - Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM,
Rosas SE, et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A consensus report by the
American Diabetes Association (ADA) and the European Association for the Study of Diabetes
(EASD). Diabetes Care. 2022;45(11):2753-2786.
doi pubmed - Riddle MC, Gerstein HC, Holman RR, Inzucchi SE, Zinman B, Zoungas S,
Cefalu WT. A1C targets should be personalized to maximize benefits while limiting risks.
Diabetes Care. 2018;41(6):1121-1124.
doi pubmed - Vijan S, Sussman JB, Yudkin JS, Hayward RA. Effect of patients' risks
and preferences on health gains with plasma glucose level lowering in type 2 diabetes mellitus.
JAMA Intern Med. 2014;174(8):1227-1234.
doi pubmed - Lachin JM, Orchard TJ, Nathan DM, DCCT/EDIC Research Group. Update on
cardiovascular outcomes at 30 years of the diabetes control and complications trial/epidemiology
of diabetes interventions and complications study. Diabetes Care. 2014;37(1):39-43.
doi pubmed - Kodama S, Horikawa C, Fujihara K, Heianza Y, Hirasawa R, Yachi Y,
Sugawara A, et al. Comparisons of the strength of associations with future type 2 diabetes risk
among anthropometric obesity indicators, including waist-to-height ratio: a meta-analysis.
Am J Epidemiol. 2012;176(11):959-969.
doi pubmed - Klein S, Gastaldelli A, Yki-Jarvinen H, Scherer PE. Why does obesity
cause diabetes? Cell Metab. 2022;34(1):11-20.
doi pubmed - Janiszewski PM, Kuk JL, Ross R. Is the reduction of lower-body
subcutaneous adipose tissue associated with elevations in risk factors for diabetes and
cardiovascular disease? Diabetologia. 2008;51(8):1475-1482.
doi pubmed - Colberg SR, Sigal RJ, Yardley JE, Riddell MC, Dunstan DW, Dempsey PC,
Horton ES, et al. Physical activity/exercise and diabetes: a position statement of the American
Diabetes Association. Diabetes Care. 2016;39(11):2065-2079.
doi pubmed - Walker RJ, Garacci E, Campbell JA, Egede LE. The influence of daily
stress on glycemic control and mortality in adults with diabetes. J Behav Med.
2020;43(5):723-731.
doi pubmed - Schrieks IC, Heil AL, Hendriks HF, Mukamal KJ, Beulens JW. The effect
of alcohol consumption on insulin sensitivity and glycemic status: a systematic review and
meta-analysis of intervention studies. Diabetes Care. 2015;38(4):723-732.
doi pubmed - Bai YL, Chiou CP, Chang YY. Self-care behaviour and related factors
in older people with Type 2 diabetes. J Clin Nurs. 2009;18(23):3308-3315.
doi pubmed - Lin EH, Katon W, Von Korff M, Rutter C, Simon GE, Oliver M,
Ciechanowski P, et al. Relationship of depression and diabetes self-care, medication adherence,
and preventive care. Diabetes Care. 2004;27(9):2154-2160.
doi pubmed - Toljamo M, Hentinen M. Adherence to self-care and glycaemic control
among people with insulin-dependent diabetes mellitus. J Adv Nurs.
2001;34(6):780-786.
doi pubmed - Weinberg Sibony R, Segev O, Dor S, Raz I. Drug therapies for
diabetes. Int J Mol Sci. 2023;24(24):17147.
doi pubmed - Hill-Briggs F, Adler NE, Berkowitz SA, Chin MH, Gary-Webb TL,
Navas-Acien A, Thornton PL, et al. Social determinants of health and diabetes: a scientific
review. Diabetes Care. 2020;44(1):258-279.
doi pubmed
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Endocrinology and Metabolism is published by Elmer Press Inc.