| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Original Article
Volume 15, Number 4, October 2025, pages 130-136

Effect of Imeglimin on Microalbuminuria and Serum Vitamin B12 Concentration in Japanese Patients With Type 2 Diabetes
Yukiyoshi Sadaa, Tomohiko Kurosua, b, Shutaro Uchiyamaa, b, Shohei Miharaa, b, Masakatsu Soneb, Yasushi Tanakaa, c
aDiabetes Center, Yokohama General Hospital, Kanagawa 225-0025,
Japan
bMetabolism and Endocrinology, St. Marianna University School of Medicine,
Kanagawa 216-8511, Japan
cCorresponding Author: Yasushi Tanaka, Diabetes Center,
Yokohama General Hospital, Yokohama, Kanagawa 225-0025, Japan
Manuscript submitted June 7, 2025, accepted August 6, 2025, published online October 6,
2025
Short title: Effect of Imeglimin in Patients With Type 2 Diabetes
doi:
https://doi.org/10.14740/jem1537
| Abstract | ▴Top |
Background: Imeglimin is a unique oral anti-diabetic agent with extra- and intra-pancreatic actions. Its safety and efficacy were demonstrated by a multicenter phase 3 trial, but its effect on albuminuria has not been fully evaluated. Metformin is the most widely used first-line anti-diabetic agent, but it partially blocks vitamin B12 (VB12) absorption in the terminal ileum. Thus, regular monitoring of serum VB12 concentration is recommended during long-term metformin treatment. Imeglimin is a small molecule synthesized from metformin via a single step chemical reaction, but whether it blocks VB12 absorption like metformin remains unclear. In this non-interventional, retrospective longitudinal study, we investigated the effects of 24 weeks of imeglimin treatment on microalbuminuria as an initial marker of albuminuria and serum VB12 concentration in Japanese patients with type 2 diabetes and microalbuminuria.
Methods: Twenty-one patients (14 men, seven women) with type 2 diabetes and microalbuminuria (30 ≤ urinary albumin-to-creatinine ratio (UACR) < 300 mg/gCre) aged 30 to 80 years (mean ± standard error (SE), 65.2 ± 2.4) were enrolled. Oral imeglimin was started at 2,000 mg daily and continued at the same dose for 24 weeks. Other anti-diabetic agents were continued at their existing dosages. Laboratory examination was performed at baseline, 12 weeks, and 24 weeks, and the effect of imeglimin on glycemic control, UACR, and serum VB12 concentration were assessed.
Results: Mean (± SE) hemoglobin A1c decreased by 0.97±0.17% from baseline to 24 weeks, and UACR also decreased significantly (100.32 ± 12.73 mg/gCre at baseline; 49.74 ± 19.32 mg/gCre at 12 weeks; 51.78 ± 21.59 mg/gCre at 24 weeks). Overall, serum VB12 concentration showed no significant change at 24 weeks. However, subgroup analysis showed a decrease in serum VB12 concentration at 12 and 24 weeks in patients receiving concomitant metformin (323.25 ± 51.75 pg/mL at baseline; 262.75 ± 40.96 pg/mL at 12 weeks; 249.75 ± 41.28 pg/mL at 24 weeks), but not in those not receiving metformin.
Conclusions: Twenty-four weeks of imeglimin treatment ameliorated glycemic control and microalbuminuria, but it decreased serum VB12 concentration in patients receiving metformin. Thus, a large-scale prospective study should be needed to confirm the results and clarify the clinical relevance in patients with type 2 diabetes.
Keywords: Imeglimin; Microalbuminuria; Vitamin B12; Metformin; Type 2 diabetes
| Introduction | ▴Top |
Type 2 diabetes mellitus is a metabolic disease characterized by chronic hyperglycemia resulting from insulin resistance and/or insulin insufficiency. It impairs quality of life and leads to significant morbidity and premature mortality [1]. Although most Caucasian patients exhibit insulin resistance (caused by obesity) while maintaining insulin secretion, in Japanese patients, the relative contribution of insulin resistance and insufficiency vary individually [2]. Thus, treatment selection for Japanese patients with type 2 diabetes should account for individual clinical characteristics, incorporating lifestyle modifications and drug interventions in line with the treatment algorithm proposed by the Japan Diabetes Society [3].
Imeglimin is a small cationic drug in the tetrahydrotriazine chemical class known as the glimins used for the treatment of type 2 diabetes. Its mechanism of action differs from that of other antihyperglycemic agents; imeglimin modulates mitochondrial function, reducing reactive oxygen species (ROS) production in systematic cells and enhancing nicotinamide adenine dinucleotide synthesis in pancreatic β cells, resulting in increased Ca2+ mobilization in the insulin secretion amplification pathway [4]. Through these unique dual actions, imeglimin ameliorates insulin resistance in the liver and skeletal muscle and increases glucose-stimulated insulin secretion from pancreatic β cells. Thus, imeglimin is expected to improve glycemic control both as monotherapy and combination with other anti-diabetic agents. In a 52-week, open-label, multicenter phase 3 trial of Japanese patients with type 2 diabetes, imeglimin was well tolerated and showed long-term safety and efficacy in both monotherapy and combination therapy [5]. However, imeglimin is currently available only in Japan, and its effects on albuminuria has not been fully evaluated.
Metformin remains the most widely used first-line oral agent for type 2 diabetes worldwide. However, it partially inhibits absorption of vitamin B12 (VB12) by interfering with calcium-dependent binding of the intrinsic factor-VB12 complex to the cubam receptor in enterocytes of the terminal ileum, which may decrease serum VB12 concentration [6, 7]. Because VB12 deficiency leads to hematologic abnormalities such as megaloblastic anemia, as well as peripheral and autonomic neuropathy, regular measurement of serum VB12 concentration is recommended during long-term metformin treatment [7, 8]. Although imeglimin differs from metformin in that it is a cyclic molecule containing a triazine ring, it is also a small molecule and can be synthesized from metformin in a single-step chemical reaction [9]. However, whether imeglimin affects intestinal VB12 absorption remains unclear, and its effects on serum VB12 concentration have not been fully evaluated.
Therefore, the present study investigated the effect of 24 weeks of imeglimin treatment on microalbuminuria (as an initial assessment of albuminuria) and serum VB12 concentration in Japanese patients with type 2 diabetes.
| Materials and Methods | ▴Top |
Participants
This single-center, non-interventional, retrospective longitudinal study included patients with type 2 diabetes who were attending the outpatient clinic at Yokohama General Hospital (Yokohama, Japan). Between December 2023 and June 2024, oral imeglimin was started at 2,000 mg daily and continued at the same dose for 24 weeks. Other anti-diabetic agents were continued at their existing dosages. The inclusion criteria were as flows: 1) aged 30 to 80 years and with a hemoglobin A1c (HbA1c) variation of less than 0.5% in the previous 6 months; and 2) chronic kidney disease (CKD) stage classified according to the American Diabetes Association (ADA) classification [10] as A2 (30 ≤ urinary albumin-to-creatinine ratio (UACR) < 300 mg/gCre, indicating microalbuminuria) and G2 (60 ≤ estimated glomerular filtration rate (eGFR) < 89 mL/min/1.73 m2) for more than 1 year. The exclusion criteria were as follows: 1) malignancy, renal disease (UACR > 300 mg/gCre and/or eGFR < 60 mL/min/1.73m2), or severe liver disease; 2) abnormal extracellular water status, such as systemic edema or dehydration; 3) presence of metals implants, such as pacemaker, plates, or stents; 4) use of methylcobalamin (VB12); 5) any other condition deemed unsuitable for the study by the attending doctors. This study was approved by the ethics committee of Yokohama General Hospital (No. 202421) and was performed in accordance with the principles of the Declaration of Helsinki. Because this was a non-interventional study, informed consent was obtained via an opt-out process on our website.
Assessment of clinical parameters and serum VB12 level
At the start of imeglimin treatment in the outpatient clinic, height and body weight (BW) were measured and body mass index (BMI) was calculated. Blood and urine samples were collected after an overnight fast at baseline and weeks 12 and 24 of imeglimin treatment for general laboratory tests. Patient characteristics such as diabetic medications were recorded. Bioelectrical impedance analysis (BIA) was performed with the body composition analyzer MC-780MA-N (Tanita Corp., Tokyo, Japan) [11]. Because abnormal extracellular water and metal implants may affect body composition measurements by BIA, patients with these conditions were excluded. The fat index (FI), as index of fat mass, was defined as total fat mass divided by height squared (kg/m2), and the skeletal muscle index (SMI), as index of muscle mass, was defined as appendicular skeletal muscle mass (ASM; the sum of the lean mass of the arms and legs) divided by height squared (kg/m2). Serum VB12 concentration were measured by Hoken Kagaku Inc. (Yokohama, Japan).
Statistical analysis
Data are expressed as mean ± standard error (SE). Changes from baseline to weeks 12 and 24 were assessed by Dunnett’s multiple comparison test. Differences in mean values between the subgroups were assessed by Student’s t-test. All analyses were performed with SPSS version 21 software package (IBM, Tokyo, Japan). Statistical significance was defined as a P value less than 0.05.
| Results | ▴Top |
We included 21 patients (14 men, seven women) with type 2 diabetes aged 37 to 80 years (mean ± SE: 65.2 ± 2.4). The baseline characteristics of the enrolled patients are shown in Table 1. The dosage of anti-diabetic agents as listed in Table 1 and other various agents were not changed during the study period. Eleven patients had mild abdominal discomfort at the beginning of treatment, but all were able to continue the 2,000 mg daily dose for 24 weeks.
 Click to view |
Table 1. Baseline Characteristics of Enrolled
Patients |
Changes in metabolic parameters are shown in Table 2. BW, BMI, FI, SMI, and systolic and diastolic blood pressure did not change over the study period. Fasting plasma glucose (FPG) and HbA1c decreased significantly from baseline to weeks 12 and 24, with decreases from baseline to week 24 of 28.0 ± 7.1 mg/dL and 0.97±0.17%, respectively. Although serum low-density lipoprotein (LDL) cholesterol and high-density lipoprotein (HDL) cholesterol did not change, serum triglycerides (TG) decreased significantly from baseline to week 24. Among the liver enzymes, aspartate aminotransferase (AST), and γ-glutamyltransferase (γ-GTP) did not change, but alanine aminotransferase (ALT) decreased significantly from baseline to weeks 12 and 24.
Click to view |
Table 2. Changes in Metabolic
Parameters |
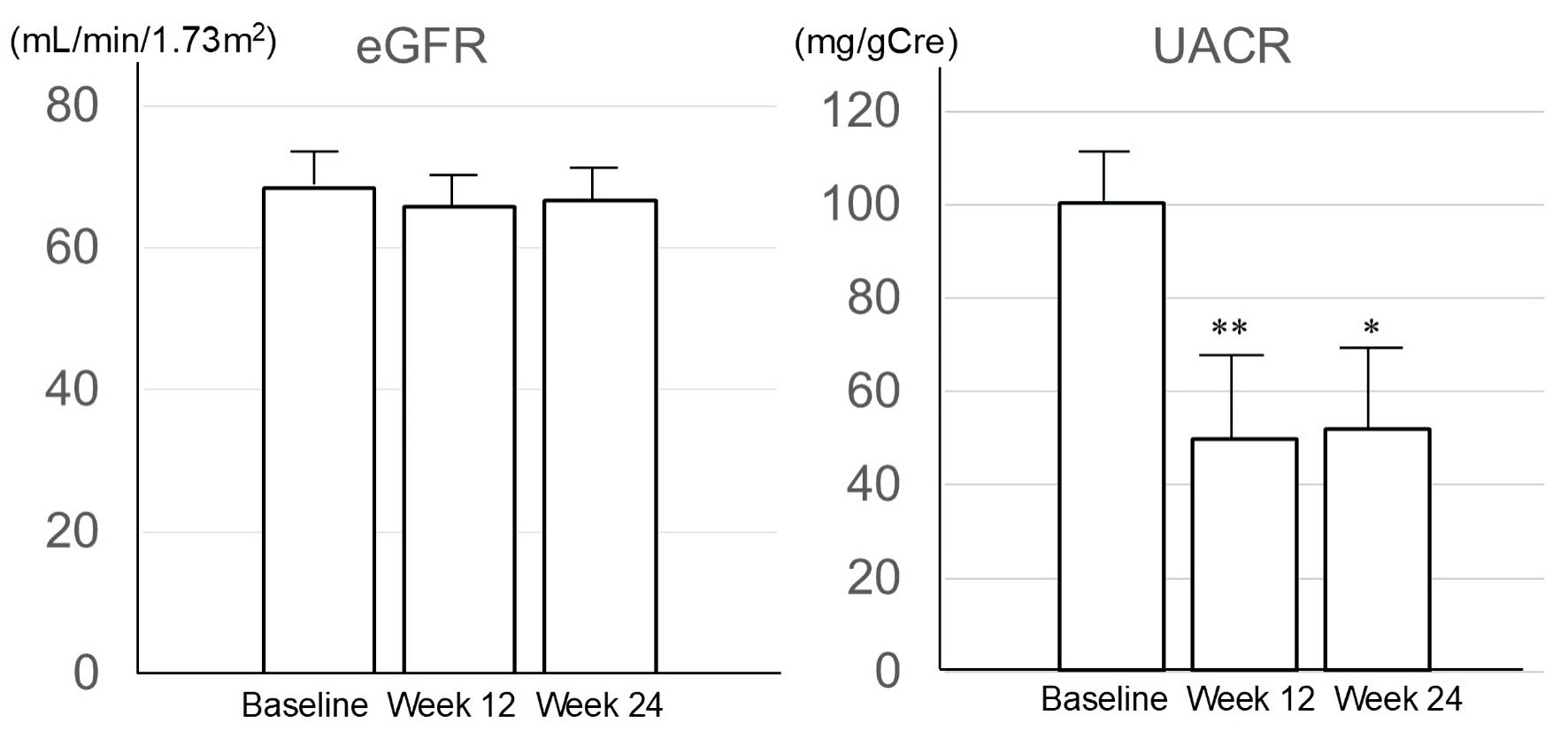
Changes in renal parameters are shown in Figure 1. Although the eGFR did not change over the study period, UACR was significantly reduced at 12 and 24 weeks. At 24 weeks, eight patients had normalized to a normoalbuminuric state (UACR < 30 mg/gCre), and the other 13 patients had improved within the range of microalbuminuria (30 ≤ UACR < 300 mg/gCre).
 Click for large image |
Figure 1. Changes of estimated glomerular filtration rate and urinary albumin creatinine ratio. Data are expressed as mean ± SE. *P < 0.05, **P < 0.01 vs. baseline. eGFR: estimated glomerular filtration rate; UACR: urinary albumin-to-creatinine ratio. |
The effect of imeglimin on red blood cell (RBC) parameters and serum VB12 concentration are shown in Table 3. Data are shown for all patients and for subgroups of patients with (n = 8) and without (n = 13) concomitant metformin. As shown in Table 4, baseline characteristics of the subgroups of patients with and without metformin were not different except for a lower proportion of women in the subgroup with metformin. Overall, RBC and hemoglobin levels decreased significantly, mean corpuscular volume (MCV) increased significantly, and VB12 concentration did not change from baseline to week 24. However, VB12 concentration decreased significantly from baseline to weeks 12 and 24 in patients receiving concomitant metformin, while it did not change in those not receiving metformin.
Click to view |
Table 3. Effect of Imeglimin on RBC Parameters
and Serum VB12 |
Click to view |
Table 4. Baseline Characteristics of Subgroups
With and Without Metformin |
| Discussion | ▴Top |
The present study demonstrated three key findings regarding the clinical effects of 24 weeks of imeglimin treatment in Japanese patients with type 2 diabetes. First, FPG and HbA1c were reduced by 28.0 ± 7.1 mg/dL and 0.97 ± 0.17%, respectively. Second, UACR decreased despite unchanged eGFR. Third, serum VB12 concentration decreased only in patients receiving concomitant metformin.
Regarding the effects on glycemic control, a phase 3 clinical trial of imeglimin reported a mean reduction in HbA1c of 0.46% in patients receiving imeglimin monotherapy and 0.56-0.92% in patients receiving combination therapy with various oral agents at 52 weeks, with the greatest reduction (0.92 %) observed in patients also receiving a dipeptidyl peptidase-4 inhibitor (DPP-4I) [5]. A recent retrospective longitudinal study of imeglimin also demonstrated a 1.1% reduction in HbA1c at 6 months [12]. Given that 81% of patients in the present study were receiving DPP-4Is, the observed HbA1c reduction is consistent with previous findings.
As shown in Table 2, we found that neither FI nor SMI, as assessed by BIA, changed over the study period, suggesting that imeglimin has a neutral effect on body composition. This finding is consistent with the recent report by Oyanagi et al [13]. Previously we reported that ALT and HbA1c were independently associated with changes in intrahepatic lipid (IHL) content, as measured by proton magnetic resonance spectroscopy [14]. In the present study, both serum ALT and HbA1c were decreased at 12 and 24 weeks, suggesting the possibility of IHL reduction.
As shown in Figure 1, UACR was reduced at 12 and 24 weeks in patients at CKD stage A2G2. Although two recent studies found no change in UACR after 6 months of imeglimin treatment, their study population included patients with macroalbuminuria [12, 15]. Because no large-scale studies on the effects of imeglimin on albuminuria in patients with type 2 diabetes have been reported, whether imeglimin can ameliorate microalbuminuria is unclear. Microalbuminuria results from increased albumin passage through the glomerular filtration barrier, which can be caused by hyperfiltration due to elevated glomerular capillary pressure (a vasodynamic factor) [16] or damage to the glycocalyx layer of glomerular capillary endothelium (a metabolic factor). The glycocalyx layer, which is composed of glycoproteins and proteoglycans, is located on the endothelial cell surface and restricts protein permeability in both systemic and glomerular capillaries [17]. In a diabetic hyperglycemic state, excessive production of ROS and proinflammatory cytokines can damage the glycocalyx layer, leading to increased permeability and microalbuminuria [17, 18]. Imeglimin improves mitochondrial function by regulating the activity of the mitochondrial respiratory chain complex and subsequently suppressing ROS production [4]. Detaille et al reported that imeglimin decreased ROS production and inhibited mitochondrial permeability transition pore opening in endothelial cells, preventing cell damage and death during hyperglycemia-induced oxidative stress [19]. In a rat model of metabolic syndrome, imeglimin treatment reduced plasma glucose and ROS production in the left ventricle and simultaneously decreased albuminuria without affecting creatininuria [20]. Together, these findings suggest that imeglimin may prevent glomerular capillary endothelial damage by suppressing ROS production, which may reduce microalbuminuria. Because microalbuminuria is a risk factor for micro- and macroangiopathy, patients at the A2G2 stage require lifestyle modification and optimal pharmacotherapy to control plasma glucose level, manage blood pressure, and prevent CKD progression [10, 17]. A consensus report by the ADA defines SGLT-2Is and glucagon-like peptide-1 receptor agonists (GLP-1Ras) as beneficial agents to prevent CKD development or progression and defines other anti-diabetic agents, not including imeglimin, as neutral [10]. Imeglimin is currently available only in Japan, and its effects on renal function remain unclear. Thus, further basic and clinical studies are needed to clarify these effects in patients with type 2 diabetes.
As shown in Table 3, serum VB12 concentration was reduced at 12 and 24 weeks only in patients receiving metformin. This finding is consistent with that of Usui et al, who recently reported that serum VB12 level was not reduced in patients treated with imeglimin monotherapy for 24 weeks [21]. Thus, imeglimin itself may not affect VB12 adsorption at the terminal ileum. Metformin is mainly absorbed in the small intestine via organic cation transporter 1 (OCT1), plasma membrane monoamine transporter, and serotonin transporter [22], and unabsorbed metformin moves to the terminal ileum and blocks VB12 absorption [6, 7]. Thus, the decrease in serum VB12 concentration is dose-dependent on metformin [23, 24], suggesting that the amount of unabsorbed metformin at the terminal ileum may be increased with higher metformin dosage, leading to lower VB12 absorption. However, the exact mechanism which VB12 decreased in the group with concomitant metformin is unclear. As imeglimin is a substrate of OCT1 [25], it may compete with metformin for absorption in the small intestine. Interestingly, co-administration of metformin (850 mg twice daily) and imeglimin (1,500 mg twice daily) for 6 days in healthy participants led to a minor reduction in plasma concentration and renal excretion of metformin [26], suggesting the possibility that more unabsorbed metformin reached the terminal ileum, potentially enhancing its inhibitory effect on VB12 absorption. However, the study did not measure fecal metformin excretion or serum VB12 concentration. Therefore, further large-scale studies are needed to clarify the effect of combined imeglimin and metformin on serum VB12 concentration and related outcomes, such as anemia or peripheral neuropathy. In this study, RBC count and hemoglobin levels were decreased at 12 weeks, and MCV was increased at 24 weeks in patients with and without concomitant metformin, suggesting that these hematological changes are not associated with metformin. A prospective study of imeglimin’s effects on erythrocytes is in progress [27] and may provide further information on hematological changes during imeglimin treatment.
The present study has several limitations. First, it was a non-interventional, retrospective longitudinal analysis of a small number of patients without a control group. At our hospital, imeglimin is typically administered to patients with reduced eGFR (< 60 mL/min/1.73m2) and/or those with receiving methylcobalamin (VB12) to treat diabetic neuropathy to prevent metformin-associated VB12 deficiency. These patients were excluded from the present study, resulting in a limited number of patients, especially in the subgroup receiving metformin. In this subgroup, the mean baseline VB12 concentration was higher than in the subgroup not receiving metformin, but the difference was not significant. The baseline VB12 concentration in the metformin subgroup ranged from 225 to 455 pg/mL, and all patients in this subgroup showed a decrease in VB12 concentration at weeks 12 and 24. Because this study was exploratory and had a limited number of patients, the generalizability of the findings may be limited. However, the results provided an interesting and important basis for further investigation. Thus, future prospective interventional studies with larger populations and control group are needed to confirm the present results. Second, UACR was evaluated with spot urine samples rather than 24-h samples. Considering the daily and diurnal variation of UACR, future studies using 24-h samples or multiple spot samples may provide more accurate assessment. Third, serum folic acid and homocysteine concentrations were not measured. Metformin may cause deficiency in folic acid in addition to VB12 [28]. Homocysteine is converted to methionine in the presence of VB12 and folic acid, and serum homocysteine concentration increases in the context of serious VB12 and folic acid deficiency. Thus, measuring VB12, folic acid, and homocysteine concentrations would provide a better understanding of the clinical relevance of reduced VB12 and folic acid. Fourth, neurological changes were not assessed. Because VB12 deficiency may be associated with peripheral neuropathy [6, 7] and cognitive impairment [29], future studies should include neurological evaluations to assess clinical significance of VB12 deficiency.
In conclusion, 24 weeks of imeglimin (2,000 mg daily) treatment improved glycemic control and reduced urinary albumin excretion in patients with type 2 diabetes and microalbuminuria. However, serum VB12 concentration was decreased only in patients receiving concomitant metformin. A large-scale prospective study is needed to confirm these results and clarify the mechanism underlying imeglimin’s effects on microalbuminuria and VB12 absorption in patients with type 2 diabetes.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Informed consent was obtained in the form of an opt-out on our website.
Author Contributions
YS designed the study, participated in data collection, performed the statistical analysis, and wrote the manuscript. TK, SU, and SM participated in data collection and statistical analysis. YT and MS designed the study and edited the manuscript. All authors approved the final version for publication.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2
diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88-98.
doi pubmed - Yoshinari M, Hirakawa Y, Hata J, Higashioka M, Honda T, Yoshida D,
Mukai N, et al. Comparison of the contributions of impaired beta cell function and insulin
resistance to the development of type 2 diabetes in a Japanese community: the Hisayama Study.
Diabetologia. 2021;64(8):1775-1784.
doi pubmed - Bouchi R, Kondo T, Ohta Y, Goto A, Tanaka D, Satoh H, Yabe D, et al.
A consensus statement from the Japan Diabetes Society (JDS): a proposed algorithm for
pharmacotherapy in people with type 2 diabetes-2nd Edition (English version). Diabetol Int.
2024;15(3):327-345.
doi pubmed - Hallakou-Bozec S, Vial G, Kergoat M, Fouqueray P, Bolze S, Borel AL,
Fontaine E, et al. Mechanism of action of Imeglimin: A novel therapeutic agent for type 2
diabetes. Diabetes Obes Metab. 2021;23(3):664-673.
doi pubmed - Dubourg J, Fouqueray P, Quinslot D, Grouin JM, Kaku K. Long-term
safety and efficacy of imeglimin as monotherapy or in combination with existing antidiabetic
agents in Japanese patients with type 2 diabetes (TIMES 2): A 52-week, open-label, multicentre
phase 3 trial. Diabetes Obes Metab. 2022;24(4):609-619.
doi pubmed - Bell DSH. Metformin-induced vitamin B12 deficiency can cause or
worsen distal symmetrical, autonomic and cardiac neuropathy in the patient with diabetes.
Diabetes Obes Metab. 2022;24(8):1423-1428.
doi pubmed - Infante M, Leoni M, Caprio M, Fabbri A. Long-term metformin therapy
and vitamin B12 deficiency: An association to bear in mind. World J Diabetes.
2021;12(7):916-931.
doi pubmed - American Diabetes Association Professional Practice C. 9.
Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2025. Diabetes
Care. 2025;48(1 Suppl 1):S181-S206.
doi pubmed - Yendapally R, Sikazwe D, Kim SS, Ramsinghani S, Fraser-Spears R,
Witte AP, La-Viola B. A review of phenformin, metformin, and imeglimin. Drug Dev Res.
2020;81(4):390-401.
doi pubmed - de Boer IH, Khunti K, Sadusky T, Tuttle KR, Neumiller JJ, Rhee CM,
Rosas SE, et al. Diabetes management in chronic kidney disease: a consensus report by the
American Diabetes Association (ADA) and kidney disease: improving global outcomes (KDIGO).
Diabetes Care. 2022;45(12):3075-3090.
doi pubmed - Uchiyama S, Sada Y, Mihara S, Sasaki Y, Sone M, Tanaka Y. Oral
semaglutide induces loss of body fat mass without affecting muscle mass in patients with type 2
diabetes. J Clin Med Res. 2023;15(7):377-383.
doi pubmed - Katsuyama H, Hakoshima M, Heshiki T, Iida S, Adachi H, Yanai H.
Real-world effectiveness of imeglimin in patients with type 2 diabetes: a retrospective
longitudinal study in Japan. Diabetes Res Clin Pract. 2024;213:111752.
doi pubmed - Oyanagi T, Kawanabe S, Tsukiyama H, Nishine A, Nakamura Y, Nakagawa
T, Kanou M, et al. The effects of imeglimin on muscle strength in patients with type 2 diabetes:
a prospective cohort study. Diabetes Ther. 2024;15(11):2323-2336.
doi pubmed - Takemoto A, Sada Y, Oyanagi T, Sasaki Y, Sone M, Tanaka Y. Alanine aminotransferase, body mass index, and hemoglobin A1c may be useful markers for monitoring changes in intrahepatic lipid content in Japanese patients with overweight or obesity and type 2 diabetes. J Endocrinol Metab. 2022;12(2):73-78.
- Uto A, Ishinoda Y, Asaga T, Tanahashi Y, Kobayashi A, Meshino H,
Okazaki M, et al. Imeglimin for type 2 diabetes mellitus: its efficacy and insight into the
potential benefit for renal and liver function. Cureus. 2024;16(8):e66322.
doi pubmed - Mogensen CE. Microalbuminuria, blood pressure and diabetic renal
disease: origin and development of ideas. Diabetologia. 1999;42(3):263-285.
doi pubmed - Satchell SC, Tooke JE. What is the mechanism of microalbuminuria in
diabetes: a role for the glomerular endothelium? Diabetologia. 2008;51(5):714-725.
doi pubmed - Yu H, Song YY, Li XH. Early diabetic kidney disease: Focus on the
glycocalyx. World J Diabetes. 2023;14(5):460-480.
doi pubmed - Detaille D, Vial G, Borel AL, Cottet-Rouselle C, Hallakou-Bozec S,
Bolze S, Fouqueray P, et al. Imeglimin prevents human endothelial cell death by inhibiting
mitochondrial permeability transition without inhibiting mitochondrial respiration. Cell Death
Discov. 2016;2:15072.
doi pubmed - Lachaux M, Soulie M, Hamzaoui M, Bailly A, Nicol L, Remy-Jouet I,
Renet S, et al. Short-and long-term administration of imeglimin counters cardiorenal dysfunction
in a rat model of metabolic syndrome. Endocrinol Diabetes Metab. 2020;3(3):e00128.
doi pubmed - Usui R, Hamamoto Y, Imura M, Omori Y, Yamazaki Y, Kuwata H, Tatsuoka
H, et al. Differential effects of imeglimin and metformin on insulin and incretin secretion-An
exploratory randomized controlled trial. Diabetes Obes Metab. 2025;27(2):856-865.
doi pubmed - McCreight LJ, Bailey CJ, Pearson ER. Metformin and the
gastrointestinal tract. Diabetologia. 2016;59(3):426-435.
doi pubmed - Kim J, Ahn CW, Fang S, Lee HS, Park JS. Association between metformin
dose and vitamin B12 deficiency in patients with type 2 diabetes. Medicine (Baltimore).
2019;98(46):e17918.
doi pubmed - Sato Y, Ouchi K, Funase Y, Yamauchi K, Aizawa T. Relationship between
metformin use, vitamin B12 deficiency, hyperhomocysteinemia and vascular complications in
patients with type 2 diabetes. Endocr J. 2013;60(12):1275-1280.
doi pubmed - Chevalier C, Fouqueray P, Bolze S. Imeglimin: a clinical pharmacology
review. Clin Pharmacokinet. 2023;62(10):1393-1411.
doi pubmed - Fouqueray P, Perrimond-Dauchy S, Bolze S. Imeglimin does not induce
clinically relevant pharmacokinetic interactions when combined with either metformin or
sitagliptin in healthy subjects. Clin Pharmacokinet. 2020;59(10):1261-1271.
doi pubmed - Osonoi T, Shirabe S, Saito M, Hosoya M, Douguchi S, Ofuchi K, Katoh
M. Comparative evaluation of clinical glycemic control markers treated with imeglimin and its
effect on erythrocytes in patients with type 2 diabetes mellitus: study protocol of a
single-arm, open-label, prospective, exploratory trial. Front Pharmacol.
2023;14:1205021.
doi pubmed - Valdes-Ramos R, Guadarrama-Lopez AL, Martinez-Carrillo BE,
Benitez-Arciniega AD. Vitamins and type 2 diabetes mellitus. Endocr Metab Immune Disord Drug
Targets. 2015;15(1):54-63.
doi pubmed - Moore EM, Mander AG, Ames D, Kotowicz MA, Carne RP, Brodaty H,
Woodward M, et al. Increased risk of cognitive impairment in patients with diabetes is
associated with metformin. Diabetes Care. 2013;36(10):2981-2987.
doi pubmed
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Endocrinology and Metabolism is published by Elmer Press Inc.