| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Review
Volume 16, Number 3, June 2026, pages 129-141

The Role of Intermittent Fasting in Modulating Hormonal Biomarkers in Women With Polycystic Ovary Syndrome: A Review
Idayakshini Ulaganathana, Iyshwarya Bhaskar Kalarania, Madhumitha Masilamania ![]() , Kaviya Manoharana, Melvin Georgea, b
, Kaviya Manoharana, Melvin Georgea, b ![]()
aCentre for Clinical Pharmacology, SRM Medical College Hospital and Research Centre, SRM Institute of Science and Technology, SRM Nagar, Kattankulathur 603203, Kanchipuram, Chennai, Tamil Nadu, India
bCorresponding Author: Melvin George, Centre for Clinical Pharmacology, SRM Medical College Hospital and Research Centre, SRM Institute of Science and Technology, SRM Nagar, Kattankulathur 603203, Kanchipuram, Chennai, TN, India
Manuscript submitted September 25, 2025, accepted March 25, 2026, published online June 10, 2026
Short title: Role of Intermittent Fasting in PCOS
doi: https://doi.org/10.14740/jem1568
| Abstract | ▴Top |
Polycystic ovary syndrome (PCOS) is a prevalent endocrine disorder among women of reproductive age, associated with hormonal imbalance, insulin resistance, and metabolic dysfunction. Recent interest has emerged around intermittent fasting (IF) as a non-pharmacological approach to managing PCOS-related symptoms. This review aims to evaluate the effects of IF interventions, including time-restricted feeding (TRF), alternate-day fasting (ADF), and the 5:2 fasting model, on hormonal, metabolic, and inflammatory biomarkers in women with PCOS. The review specifically focuses on insulin resistance indices (e.g., Homeostatic Model Assessment for Insulin Resistance), androgen-related markers such as testosterone and sex hormone-binding globulin (SHBG), gonadotropins (luteinizing hormone (LH) and follicle-stimulating hormone (FSH)), and inflammatory biomarkers reported in human studies and relevant mechanistic research. Evidence suggests that IF, particularly TRF, significantly improves insulin sensitivity, reduces hyperandrogenism, and supports weight loss, all of which are critical in PCOS management. IF also influences circadian rhythms, reproductive hormone regulation, and inflammatory markers such as C-reactive protein (CRP) and tumor necrosis factor-alpha (TNF-α). Some studies indicate enhanced menstrual regularity and ovulation with IF regimens. However, hormonal changes in estrogen, LH, and FSH levels remain inconsistently reported. Molecular mechanisms involve activation of AMP-activated protein kinase (AMPK), sirtuin 1 (SIRT1), and suppression of the mechanistic target of rapamycin (mTOR) pathway, contributing to improved metabolic and hormonal balance. IF shows promise as an adjunct therapy for managing PCOS by targeting metabolic, hormonal, and reproductive dysfunctions. Nevertheless, further long-term, large-scale human trials are necessary to establish standardized IF protocols and confirm safety and efficacy.
Keywords: Polycystic ovary syndrome; Intermittent fasting; Time-restricted feeding; Hyperandrogenism; Insulin resistance; Hormonal biomarkers; Metabolic health; Reproductive function
| Introduction | ▴Top |
Polycystic ovary syndrome (PCOS) is linked to increased ovarian androgen production, which is characterized by an accumulation of ovulated follicles in the ovaries. There is not a single diagnostic standard that can be used to confirm a clinical diagnosis of PCOS. It is identified by ultrasound evidence of hyperandrogenism or polycystic ovaries [1]. PCOS was first determined to be the most common cause of oligo-ovulatory infertility in 1935. Endometrial cancer, infertility, abnormal uterine bleeding, and certain metabolic disorders such as diabetes mellitus, insulin resistance (IR), hypertension, dyslipidemia, and cardiovascular disease are all more common in these individuals [2]. PCOS is the most prevalent hormonal disorder among women of reproductive age [3]. Globally, the 25–29 age group has the highest occurrence of PCOS, followed closely by the 20–24 range. While PCOS affects women throughout reproductive age (15–49), its burden is most concentrated in early to mid-reproductive years, reflecting peak hormonal activity and metabolic vulnerability [4]. Deswal et al conducted a systematic review examining the prevalence of PCOS in India, revealing that rates range from 3.7% to 22.5%. This variation is attributed to differences in diagnostic methods, demographic characteristics, and the context of individual studies [5]. The high prevalence of PCOS among young women in Delhi NCR is primarily attributed to urban lifestyle factors such as increased stress, sedentary behavior, dietary habits, and sociodemographic influences, including age (≥ 20 years), higher education, nuclear family structure, and specific ancestral backgrounds. These factors collectively contribute to a greater risk of developing PCOS in urban settings compared to other regions in India [6].
PCOS can be defined by certain diagnostic criteria, but the most pertinent criteria for PCOS diagnosis are still up for debate. In 1935, Stein and Leventhal were the first to describe PCOS as a hormonal disorder associated with infrequent ovulation and infertility in women. Despite being the most widely used PCOS categorization, the Rotterdam 2003 criteria are not universally recognized [7]. According to the Rotterdam criteria established in 2003 by European Society for Human Reproduction and Embryology (ESHRE) and American Society for Reproductive Medicine (ASRM), a diagnosis of PCOS can be made if an individual presents with any two of the following three features: infrequent or absent ovulation, elevated androgen levels, or the presence of polycystic ovaries. This diagnostic framework is one of the most widely used standards for identifying PCOS both clinically and biochemically. Both environmental and genetic factors contribute to the development of PCOS. Genetic risk factors include early fetal programming, advanced pubertal onset, and having first-degree relatives with a history of the condition. Environmental causes include obesity, advanced glycation end products (AGEs), consuming junk food heavy in fat, salt, and sugar, and not exercising [8]. The modified Rotterdam criteria should be used, according to which PCOS can be identified if any two of the following conditions are met: 1) oligo-anovulation evidence, 2) clinical or biochemical hyperandrogenism, and 3) polycystic-looking ovarian morphology on ultrasound, while ruling out other pertinent disorders [8].
The objective of this review is to synthesize current evidence regarding the impact of intermittent fasting (IF) protocols on hormonal and metabolic biomarkers in women with PCOS. Specifically, this review evaluates the effects of different IF approaches including time-restricted feeding (TRF), alternate-day fasting (ADF), and the 5:2 diet on IR indices, androgen-related biomarkers (testosterone and sex hormone-binding globulin (SHBG)), gonadotropins, and inflammatory markers associated with PCOS. The review primarily focuses on findings from human studies involving women with PCOS, while also incorporating mechanistic and experimental evidence to provide a biological context.
| Literature Search Strategy | ▴Top |
A structured narrative review of the literature was conducted to examine the effects of IF on hormonal and metabolic biomarkers in women with PCOS. Relevant articles published between January 2000 and January 2025 were identified through searches of electronic databases including PubMed, Scopus, Web of Science, and Google Scholar.
The search strategy used combinations of keywords and Medical Subject Headings (MeSH) such as “polycystic ovary syndrome,” “PCOS,” “intermittent fasting,” “time-restricted feeding,” “alternate-day fasting,” “5:2 diet,” “insulin resistance,” “androgens,” “hormonal biomarkers,” and “metabolic biomarkers.” Boolean operators (AND/OR) were used to refine the search.
Studies were considered eligible if they evaluated IF or fasting-related dietary interventions and reported metabolic, hormonal, or inflammatory outcomes relevant to PCOS. Human clinical studies involving women diagnosed with PCOS were prioritized. Additional mechanistic studies and relevant experimental research were also included to provide biological context for the metabolic and endocrine mechanisms discussed.
Articles not published in English, conference abstracts without full text, duplicate records, and studies unrelated to PCOS or IF were excluded.
As this work represents a structured narrative review, formal systematic review procedures such as PRISMA flow diagrams, independent dual screening, and formal risk-of-bias assessment were not performed. However, the included literature was critically evaluated to synthesize current evidence regarding the metabolic and hormonal effects of IF in PCOS.
| Clinical Manifestations of PCOS | ▴Top |
The formation of many immature follicles is one of the characteristic polycystic ovarian morphological alterations of PCOS, a common reproductive endocrine condition [9, 10]. This medical disorder, which typically manifests as secondary amenorrhea or oligomenorrhea, interferes with the regularity of the menstrual cycle. PCOS has a major impact on reproductive function and can cause infertility and miscarriage in extreme circumstances [11]. PCOS has a complex etiology that includes elevated pituitary luteinizing hormone (LH) and decreased gonadotropin-releasing hormone (GnRH) pulsatility. Chronic low-grade inflammation, obesity, IR, high androgen levels secretion, and elevated androgenic hormones are a critical diagnostic marker of hyperandrogenism, which causes clinical symptoms such as baldness, hirsutism, and acne. Elevated androgenic hormones that result in clinical symptoms are a crucial diagnostic characteristic of hyperandrogenism [11–13]. Illustrations of the risk factors and symptoms are given in Figure 1.
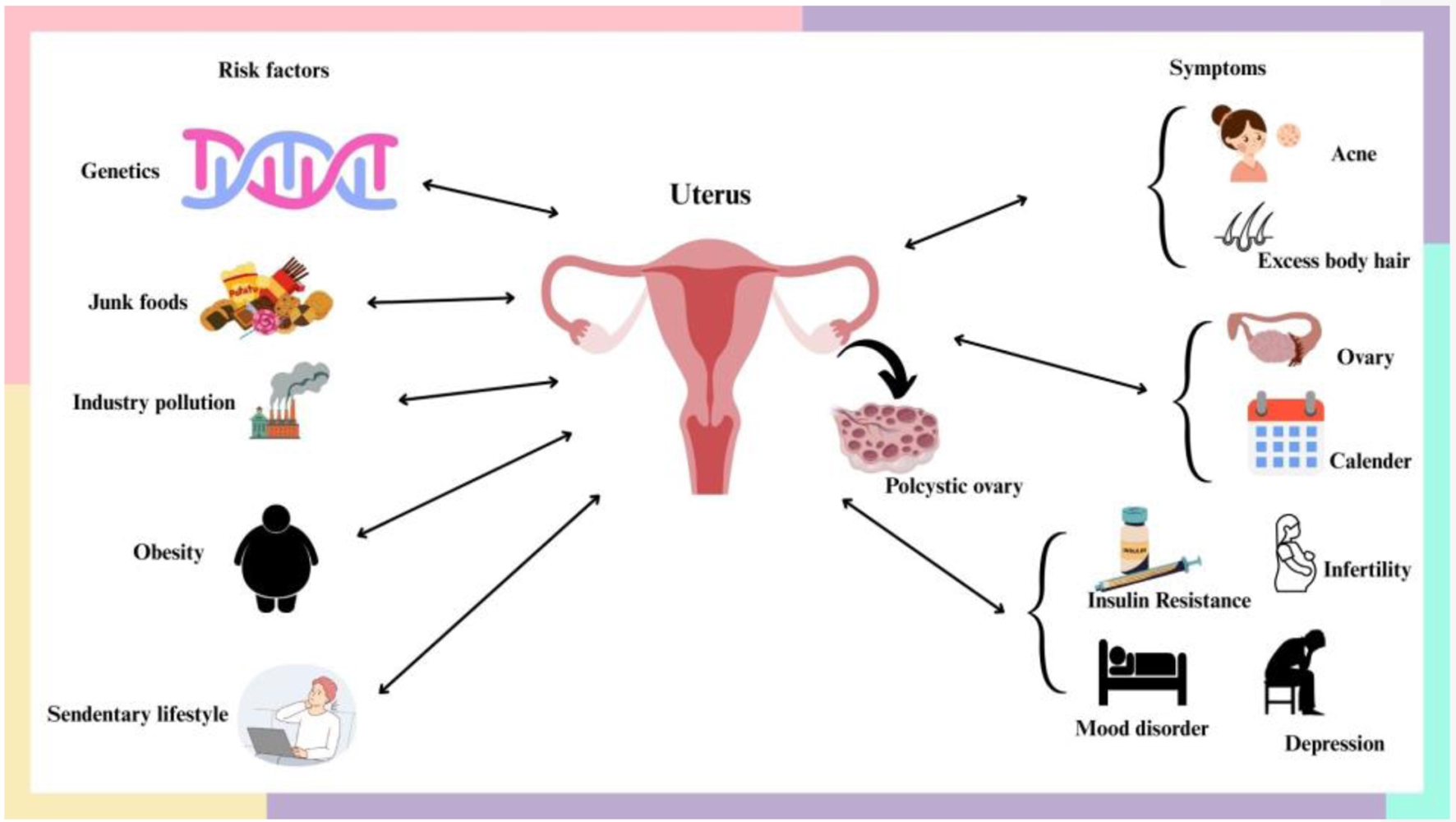 Click for large image | Figure 1. An illustration depicting the risk factors and symptoms associated with the development of PCOS in women. Genetic, lifestyle, and environmental factors contribute to hormonal imbalance, insulin resistance, and ovarian dysfunction, resulting in polycystic ovaries and characteristic reproductive, metabolic, and psychological manifestations. |
In women, androgens play a vital role in maintaining sexual health, muscle strength, and bone density. These hormones, such as testosterone, dihydrotestosterone, dehydroepiandrosterone sulphate (DHEA-S), dehydroepiandrosterone (DHEA), and androstenedione (ANSD), are produced from three primary sources: approximately 25% by the ovaries, 25% by the adrenal glands, and the remaining 50% by peripheral tissues. The ovaries create the majority of testosterone, the adrenal gland and ovaries produce ANSD equally, and the adrenal gland produces DHEA-S alone [14]. IR is commonly observed in individuals with PCOS, leading to reduced cellular sensitivity to insulin and impaired glucose absorption and metabolism. This condition is closely linked to the development of type 2 diabetes and may also contribute to obesity. In PCOS, the ovaries are the primary source of excess androgens. As a result, elevated levels of testosterone particularly in its free form, unbound to SHBG serve as the most reliable diagnostic indicator of hyperandrogenism [14].
Other characteristics of PCOS include metabolic (increased risk and prevalence of type 2 diabetes and cardiovascular disease), psychological (anxiety, sadness, and poor quality of life (QoL)), and reproductive (subfertility, infertility, and pregnancy problems) [15]. The etiology of PCOS is still not fully known, despite the condition’s well-established negative health effects. Intrinsic IR, which is particular to PCOS and is linked to a dysregulated response to insulin in peripheral tissues that are metabolically active, and extrinsic IR, which is linked to obesity and occurs when weight gain exacerbates PCOS pathology, are two potential mechanisms underlying PCOS [15]. To make things even more complicated, PCOS is associated with food cravings and binge-eating symptoms [16], which may exacerbate endocrine disruptions and body fat accumulation while also encouraging negative body image, self-blame, and associated psychosocial worries [17].
Preeclampsia, gestational diabetes mellitus (GDM), and an elevated risk of preterm birth are among the pregnancy-related conditions that are associated with PCOS. Infants born to mothers with PCOS may be more likely to die and be admitted to neonatal intensive care units [18]. Women with PCOS frequently experience disrupted menstrual cycles due to anovulation (lack of ovulation) and hormonal imbalances, including elevated LH levels and androgens like testosterone. These disruptions can lead to cycles longer than 35 days, fewer than eight periods per year, or complete absence of menstruation. There is an observed association between PCOS and autoimmune condition such as thyroid dysfunction. Women with PCOS have higher rates of positive thyroid autoantibodies and subclinical hypothyroidism compared to the general population [19].
| Management of PCOS | ▴Top |
PCOS management requires a multimodal strategy based on each patient’s symptoms and health objectives. This multifaceted approach involves combination of lifestyle modifications with pharmacological interventions [20]. Lifestyle modification is the important strategy to manage PCOS. Dietary interventions such as calories-restricted diets, high-protein diet, and regular physical activities have been demonstrated to improve IR, hormonal balance, and menstrual regularity that are commonly observed physiological conditions in PCOS. Jungari et al conducted a retrospective cohort observational study on demonstration of a combination of lifestyle modifications, metformin therapy, and enhanced adherence counselling in central India that led to significant improvements in body mass index (BMI), blood sugar levels, and hormonal profiles, with 91% of women experiencing regular menstrual cycles after 6 months of intervention [21]. Despite the established benefits of lifestyle management, its implementation in clinical practice remains suboptimal. A study from Bosnia and Herzegovina highlighted that only 34.8% of physicians initiated treatment plans based solely on lifestyle measures, underscoring the need for enhanced education and support for healthcare providers to effectively counsel patients on lifestyle interventions [22]. Prior to initiation of any pharmaceutical therapies, all women with PCOS must receive non-pharmacological guidance. This is due to the fact that non-pharmacological treatments like diet and exercise are the only ones that can help the majority of women with PCOS. However, the course of treatment would mostly depend on the patient’s decisions and the severity of their health [23]. There are currently no proven treatments or cures for this illness; instead, symptomatic therapy with a variety of medicines, such as oral antidiabetics, contraceptives, or antiandrogens, is the standard approach following lifestyle adjustment and additional advice. Repurposing medications is a wonderful option because it may help PCOS [24]. Dietary intervention is therefore essential for controlling PCOS and improving the syndrome in women. It has been demonstrated that dietary interventions like calorie restriction (CR), time restriction in feeding (e.g., IF, ADF, 5:2-day approach), high-protein diet, high-fiber diet, diets rich in omega-3 fatty acids, ketogenic diets, Mediterranean diets, and foods high in antioxidants can help manage PCOS [25, 26].
The potential advantages of IF, especially TRF, in the treatment of PCOS have drawn attention [27]. A 24-h fast on alternate days, a 16-h fast every day, or a full 24-h fast twice a week on non-consecutive days are all considered forms of IF. Thus, IF can be used to describe a duration of fasting that ranges from 12 to 20 h [28]. As an alternative to traditional daily CR, IF has gained popularity. IF strategies include ADF and restricting food intake to specific times of the day [29]. Dietary treatments for PCOS have gained popularity recently in endocrine and reproductive studies. Given that between 38% and 88% of women with PCOS are fat or overweight [30], the significance of food in PCOS is also emphasized by the International Evidence-based Guideline for the Assessment and Management of PCOS, which suggests dietary and exercise therapies as the first line of treatment for this population [31].
A number of diets have been suggested thus far for the treatment of PCOS, including the low-glycemic index diet [32], DASH diet [33], Mediterranean diet [34], low-carb diet [35], and ketogenic diet [36]. To provide the most effective specific dietary intervention for enhancing PCOS health outcomes, there is an information vacuum. IF’s impact on hormonal indicators in PCOS-afflicted women is still mostly unclear. We carried out this review in order to fill up this knowledge vacuum on the impact of IF on hormonal indicators in PCOS-afflicted women.
| Effect of IF on Metabolism and Hormonal Balance in PCOS | ▴Top |
PCOS is a hormonal disorder often linked to IR, hyperandrogenism, obesity, and chronic inflammation. There are several types of IF protocol, including TRF, ADF, 5:2 diet, and Ramadan fasting, each exerting distinct metabolic effects in women with PCOS. Metabolic impacts of IF in PCOS are summarized in Table 1 [27, 37, 38]. TRF has a positive metabolic effect such as improvement in insulin sensitivity, reduces androgens, enhances menstrual regularity, and supports weight and fat loss. The 5:2 diet also helps in reducing insulin levels, promotes fat loss, and may improve lipid profile. ADF improves glucose and lipid metabolism, aids in weight loss, and may be harder to sustain. The 24-h fast (1–2 times per week) promotes fat oxidation and reduces inflammation, but there is limited evidence on this IF protocol.
 Click to view | Table 1. Summary of IF Protocols and Their Metabolic Effects in PCOS |
A reduction in androgen levels, particularly in individuals with hyperandrogenism such as in PCOS, can have significant positive effects on reproductive outcomes. Androgens (e.g., testosterone, androstenedione) are male sex hormones present in both men and women, but excess levels in women can cause anovulation (lack of ovulation), irregular menstrual cycles, infertility, hirsutism, acne, and alopecia. Reduction in these levels can restore hormonal balance and improve reproductive function. Elevated androgens, such as testosterone, are a hallmark of PCOS. In women who have reproductive hormones and fertility issues, TRF significantly improves these aspects. “A study on the effect of intermittent fasting on fertility: a focus on polycystic ovary syndrome and reproductive outcomes in women - a systematic review” was carried out by Velissariou et al. In women with PCOS, IF, especially TRF, improves fertility and reproductive health. TRF enhanced insulin sensitivity, decreased inflammation, decreased body weight, and decreased androgen index, all of which improved reproductive results [37].
Few studies have demonstrated that feeding animals with PCOS under time restrictions improves their metabolic and endocrine profiles. TRF has demonstrated beneficial effects on diseases of glycolipid metabolism and obesity. In order to demonstrate to the general public that TRF had some beneficial effects on people with PCOS, they sought to investigate the effects of TRF in mouse models in comparison to ad libitum. They found that TRF improved the metabolic and endocrine profiles of mice with PCOS [38].
IF, particularly TRF, has shown improvement in menstrual cycle regularity and ovulatory function in women with PCOS. A study titled “Eight-hour time-restricted feeding improves endocrine and metabolic profiles in women with anovulatory polycystic ovary syndrome” shows that 73.3% of the study participants experienced improved menstrual cycles after a 5-week TRF intervention. TRF also reduced chronic inflammation (hs-CRP levels) among the study participants [39].
Short-term TRF does not appear to significantly affect estrogen, LH, or follicle-stimulating hormone (FSH) levels in premenopausal women. The study titled “Effect of time restricted eating on sex hormone levels in premenopausal and postmenopausal women” showed no significant effects on androgens and SHBG levels in premenopausal women, while DHEA decreased during TRF intervention [40].
| Association Between Obesity and PCOS and Impact of IF | ▴Top |
One of the most clinically proven significant links with PCOS is obesity. Obesity is an inflammatory condition in which the excessive body fat deposition disrupts the hormonal and metabolic balance [41]. Obesity is one of the risk factors contributing to the development of PCOS. The connection between obesity and PCOS is multifactorial, involving genetic, hormonal, and environmental elements that influence IR, inflammation, and androgen production [42, 43]. Schematic illustrations of the etiology and clinical feature are given in Figure 2. IR can promote the development of hyperinsulinemia, which promotes hyperandrogenism and chronic anovulation. Around 52–64% of women with PCOS exhibit abdominal fat accumulation, which is independently associated with metabolic abnormalities such as IR [44].
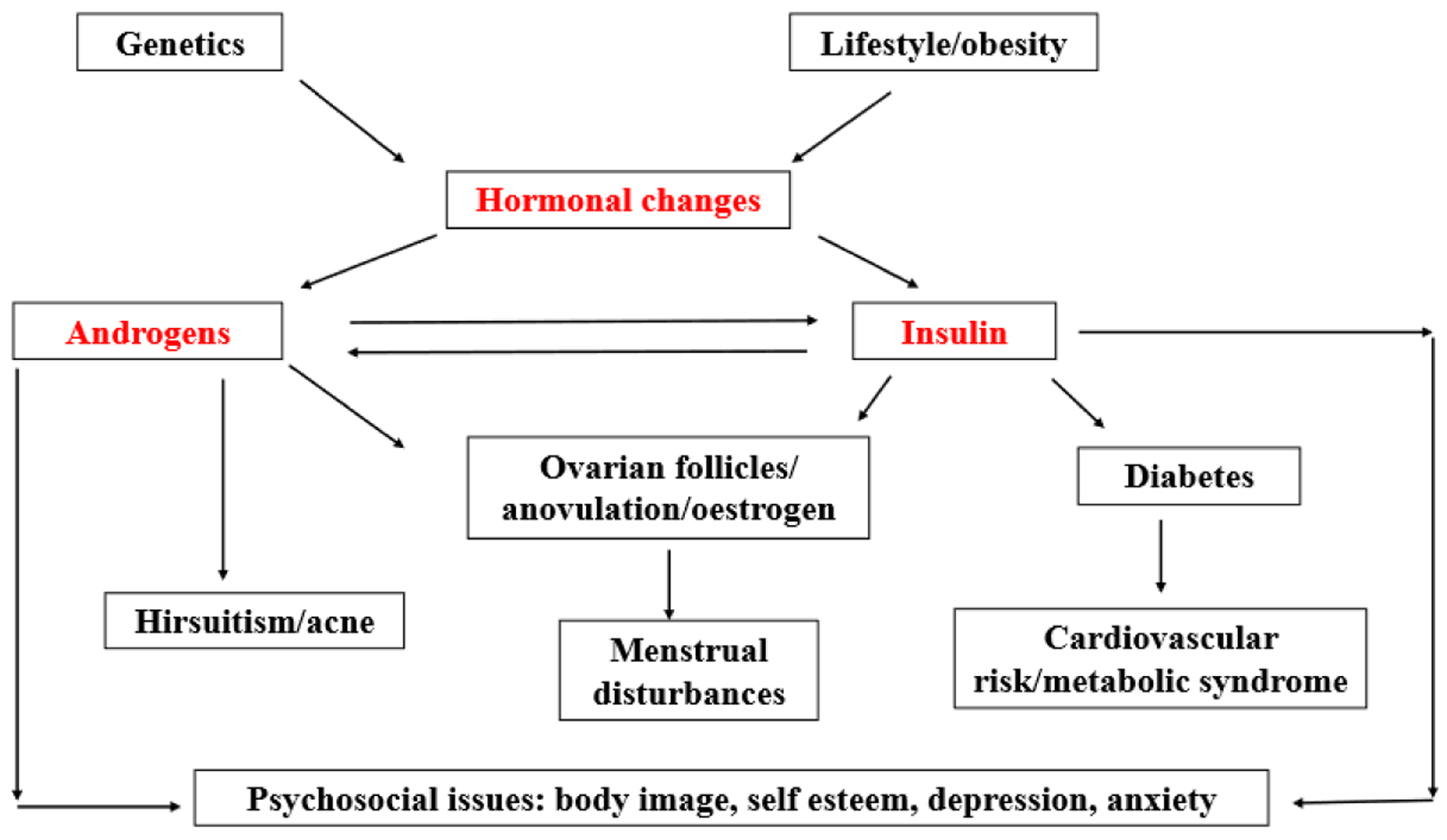 Click for large image | Figure 2. Diagram showing the etiology and clinical characteristics of polycystic ovarian syndrome (PCOS), including its metabolic, reproductive, and psychological aspects. “Hormonal changes,” “Androgens,” and “Insulin” represent key regulatory or pathological factors in the development. |
Inflammatory markers are generally elevated in individuals with obesity. The elevation indicates the presence of low- to high-grade chronic inflammation in the individual’s body. Obese women with PCOS normally show increased levels of inflammatory markers such as C-reactive protein (CRP), tumor necrosis factor-alpha (TNF-α), interlukin-6 (IL-6), monocyte chemoattractant protein-1 (MCP-1), and plasminogen activator inhibitor-1 (PAI-1). CRP is an acute phase protein which is produced by liver in response to inflammation. Several research studies have shown elevated CRP levels in women with PCOS, especially those who are obese. Studies on circulating inflammatory markers in PCOS provide a comprehensive analysis of serum inflammatory markers and highlight significant elevations in CRP levels compared to controls. The findings prove that these elevations are not influenced by obesity, indicating a persistent, low-grade inflammatory condition in PCOS [45].
A pro-inflammatory cytokine implicated in IR and inflammation of adipose tissue is TNF-α. In obese women, TNF-α is found in elevated levels in adipose tissues contributing to IR and hyperandrogenism. Studies found elevated serum TNF-α in obese PCOS patients compared to lean PCOS and controls, which suggests that chronic low-grade inflammation may be present in PCOS regardless of body weight [46]. IF could help mitigate chronic inflammations, IR, and hyperandrogenism through multiple mechanisms such as improvement in insulin sensitivity, reduction in inflammatory markers, weight loss, body composition improvements, and hormonal regulation [47].
| Evidence From Human Studies in PCOS | ▴Top |
Current clinical evidence evaluating IF in women with PCOS remains limited but growing. Most available studies primarily report improvements in metabolic parameters such as body weight, insulin sensitivity, and lipid profiles. These metabolic improvements may indirectly influence endocrine disturbances associated with PCOS, including hyperandrogenism and ovulatory dysfunction. Therefore, the findings from human studies in PCOS populations provide the most clinically relevant evidence for understanding the potential role of IF in managing PCOS-related metabolic and hormonal abnormalities.
| Molecular Pathway of IF in PCOS | ▴Top |
IF has been investigated for possible advantages in various health conditions, including PCOS. Adenosine monophosphate-activated protein kinase (AMPK), a crucial cell energy sensor, is known to be stimulated by IF. Since IR is a prevalent problem in PCOS, AMPK activation can increase insulin sensitivity, which is essential for controlling its symptoms [48]. During fasting, the body experiences a decrease in energy availability. This energy depletion leads to an increase in the adenosine monophosphate to adenosine triphosphate (AMP/ATP) ratio. When AMP levels rise, AMPK is activated as it senses low energy status in the cell. Once activated, AMPK phosphorylates and inhibits acetyl-CoA carboxylase (ACC), which is involved in fatty acid synthesis. This inhibition promotes fatty acid oxidation, allowing the body to utilize fat stores for energy, which is particularly beneficial during fasting. AMPK activation also encourages the translocation of glucose transporter type 4 (GLUT4) to the cell membrane, which increases the absorption of glucose in muscle and fat tissues. An illustration of the molecular pathway of IF in PCOS is given in Figure 3.
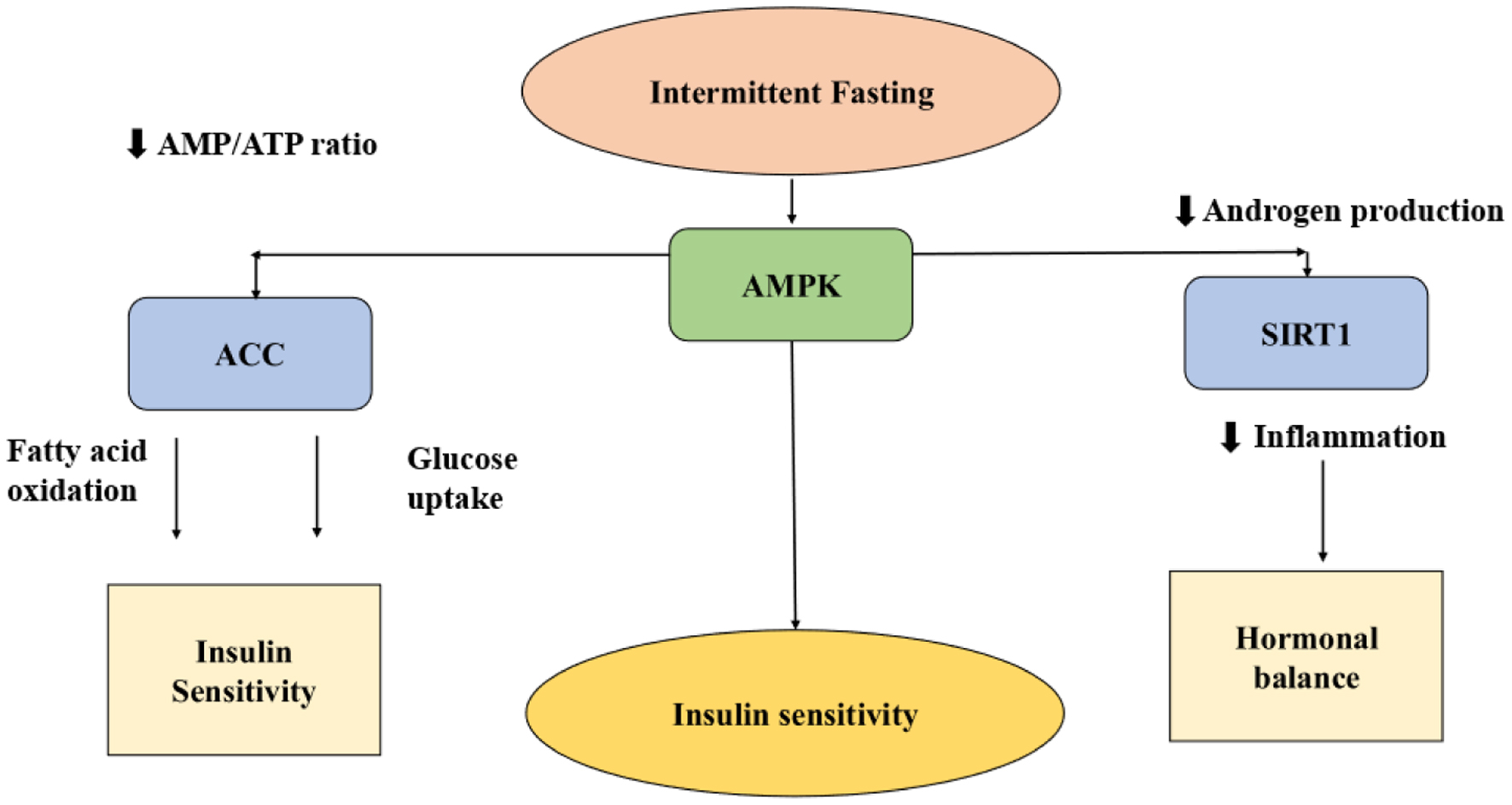 Click for large image | Figure 3. Illustration of the molecular pathway of IF in PCOS; AMPK: adenosine monophosphate-activated protein kinase; ACC: acetyl-CoA carboxylase; AMP/ATP ratio: adenosine monophosphate to adenosine triphosphate; SIRT1: sirtuin 1. |
This process helps improve insulin sensitivity, which is crucial for metabolic health. By promoting fatty acid oxidation and inhibiting lipogenesis, AMPK activation helps reduce lipid accumulation in tissues. This is important for preventing lipotoxicity, which can contribute to IR and other metabolic disorders. The major studies do not specifically mention how an IF could help in activating AMPK; however, they highlight the importance of dietary strategies in activating AMPK. For instance, combining CR with omega-3 fatty acids and polyphenols can further enhance AMPK activity, leading to improved metabolic outcomes. AMPK is activated during IF primarily through energy depletion, leading to a higher AMP/ATP ratio. This activation promotes various metabolic processes that enhance insulin sensitivity and fat oxidation, contributing to overall metabolic health [49, 50]. AMPK activation enhances insulin sensitivity and promotes glucose uptake in tissues, which is particularly beneficial for individuals with IR, a common issue in PCOS. This activation can help regulate metabolic processes and improve hormonal balance.
Sirtuins are a family of proteins that play a role in cellular regulation, including metabolism and aging. IF may enhance the activity of sirtuins, which can help in regulating glucose metabolism and reducing inflammation, both of which are beneficial for women with PCOS. SIRTs, particularly SIRT1, are known to regulate metabolic processes. They help in the modulation of energy metabolism, which is crucial during IF. By enhancing mitochondrial function and promoting fat oxidation, SIRTs can improve metabolic health, which is often impaired in conditions like PCOS. IF has been shown to improve insulin sensitivity, a key factor in managing PCOS. SIRT1 plays a role in this process by deacetylating proteins involved in insulin signaling pathways, thereby enhancing the body’s response to insulin. Chronic inflammation is a common feature of PCOS. SIRTs, especially SIRT1 and SIRT3, have anti-inflammatory properties. They can modulate inflammatory responses, which may help alleviate some of the inflammatory symptoms associated with PCOS. SIRT1 can influence the secretion of hormones like leptin and adiponectin, which are important for maintaining energy balance and metabolic health. IF induces a mild stress response that activates SIRTs. This activation can enhance cellular repair mechanisms and promote longevity, which is beneficial for overall health and may help in managing PCOS symptoms [51]. Although these molecular mechanisms have been primarily demonstrated in experimental and metabolic studies, they provide biological plausibility for the metabolic improvements observed in clinical studies involving women with PCOS.
The development and metabolism of cells are influenced by the mechanistic target of rapamycin (mTOR) pathway. IF can inhibit mTOR signaling, which may help in reducing the overproduction of androgens (male hormones) that is often seen in PCOS. This inhibition can lead to improved ovarian function and reduced symptoms. mTOR is a crucial regulator of cell growth and metabolism, responding to nutrient availability and energy status. During IF, mTOR activity is typically reduced, which promotes autophagy, a process that helps in cellular repair and maintenance. This reduction in mTOR signaling during fasting periods is essential for metabolic health and can help in managing conditions like obesity and IR, which are often linked to PCOS. IF can improve glucose homeostasis by modulating mTOR signaling. For instance, studies have shown that high mTORC1 activity can lead to IR, while periods of fasting can help reset this signaling pathway, improving insulin sensitivity. This is particularly relevant for individuals with PCOS, who often experience IR. PCOS is characterized by hormonal imbalances and metabolic issues, including IR. By regulating mTOR signaling, IF may help improve insulin sensitivity and reduce hyperinsulinemia, which are common in PCOS. The biphasic effect of mTORC1 signaling, where initial activation can be beneficial but prolonged activation leads to dysfunction, mirrors the metabolic challenges faced in PCOS. IF promotes a balance in mTOR activity, which is crucial for muscle health. Proper muscle function is important for overall metabolism and can influence the symptoms of PCOS. Enhanced autophagy during fasting helps in the turnover of damaged cells, supporting better muscle function and metabolic health. Given the role of mTOR in regulating various metabolic processes, targeting mTOR signaling through dietary interventions like IF could be a promising strategy for managing PCOS. This approach may help in restoring normal metabolic function and improving reproductive health [52]. IF can influence the endocrine system by modulating hormone levels, including growth hormone and insulin-like growth factor 1 (IGF-1). These changes can help in restoring hormonal balance in women with PCOS, potentially alleviating symptoms such as irregular menstrual cycles and weight gain. Chronic inflammation is a common feature of PCOS. IF has been shown to reduce inflammatory markers, which can help in managing PCOS symptoms and improving overall health.
| Impact of IF on Obese Women With PCOS | ▴Top |
Obesity exacerbates IR, hyperandrogenism, and chronic inflammation in PCOS, and IF helps modulate these factors through multiple mechanisms. An academic institution in Chicago, Illinois, conducted a randomized clinical research from 2011 to 2015 to evaluate the impact of ADF on weight loss, weight maintenance, and cardio-protection in obese people with metabolically sound bodies, suggesting that ADF was effective for weight loss and fat reduction in obese adults. This study involved approximately 86 women and 16 men. The findings suggest that the majority of participants were women, who achieved significant weight loss and fat reduction, with potential improvements in PCOS symptoms.. Therefore, the study concluded that ADF could improve PCOS symptoms in women with PCOS [53].
In a randomized 6-month study, Trepanowski et al examined the effects of intermittent energy restriction (IER) and continuous energy restriction (CER) on weight loss, insulin sensitivity, and risk factors for metabolic diseases in 107 premenopausal women who were overweight or obese. There was no discernible difference in the weight loss that both groups experienced (IER: −6.4 kg; CER: −5.6 kg). Similar improvements were seen in metabolic and hormonal parameters following both therapies. These benefits included increases in SHBG and IGF binding proteins and decreases in leptin, free androgen index, C-reactive protein, low-density lipoprotein (LDL) cholesterol, triglycerides, and blood pressure. IR and fasting insulin, however, improved marginally more with IER (both statistically significant, P = 0.04). These results imply that, with only slight improvements in insulin-related outcomes, IER is just as successful as CER at promoting weight loss and improving important health indicators. As a result, IER might be regarded as a practical and adaptable substitute for CER in this population’s weight management and disease risk reduction [54].
In an 8-week clinical research, Kalam et al [40] examined how TRE affected the levels of sex hormones in obese premenopausal and postmenopausal women. The study implemented a 4–6 h daily eating window and observed outcomes related to weight and hormone changes. In premenopausal women, TRE led to a modest 3% weight loss, with no significant changes in key reproductive hormones such as testosterone, androstenedione, and SHBG. However, there was a notable decrease in DHEA levels (∼14%), although they remained within the normal physiological range. Since DHEA is a precursor for estrogen and androgens, its reduction may hold implications for hormone-sensitive conditions, including breast cancer.
This study provides reassurance that short-term TRE is hormonally safe for premenopausal women with obesity, showing no adverse impact on androgenic or binding proteins. These findings are particularly relevant for populations such as women with PCOS, where hormonal balance and metabolic control are critical. Despite these promising outcomes, the authors point up a number of drawbacks, including a limited sample size, a brief study period, and no menstrual cycle tracking, in premenopausal participants. As a result, while initial findings suggest that TRE is a viable and non-disruptive dietary approach for obese women, further large-scale, long-term studies are warranted to confirm its safety and effectiveness, especially among women with reproductive endocrine disorders like PCOS [55]. A systematic review suggests that TRF could improve IR in those with PCOS and the study concluded that there is no strong evidence supporting the effectiveness of time-restricted eating to reduce insulin in PCOS patients. Although findings from other populations suggest potential benefits, high-quality, well-designed studies are needed to confirm its efficacy in PCOS [55].
Because of its impact on insulin sensitivity and metabolic health, IF, especially TRE, has drawn attention as a possible non-pharmacological treatment for PCOS. Dietary measures are essential for women with PCOS since they frequently have hyperinsulinemia, IR, and an elevated risk of type 2 diabetes. Gray et al conducted a randomized controlled trial on the impact of IER on weight loss and diabetes risk markers in women with a history of gestational diabetes. Both IER and CER significantly reduced weight, with IER producing a marginally higher reduction. Both groups’ HbA1c, fasting insulin, fasting plasma glucose, and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) scores improved. Both groups showed initial improvements in metabolic health indicators, particularly in the early phase of the intervention, suggesting benefit in reducing future diabetes risk. Physical activity levels slightly decreased over the 12 months in both groups, and sleep quality improved modestly, suggesting potential benefits to overall well-being [56].
According to Floyd et al [55], although theoretical benefits of IF are supported by its impact on metabolic flexibility, insulin regulation, and inflammation in other populations, there is insufficient direct evidence in PCOS. Only one controlled study focusing on Ramadan fasting was included in the systematic review and showed no significant effect on insulin or glucose levels. However, a non-controlled pilot study involving a 16:8 TRE regimen showed reductions in fasting insulin, HOMA-IR, body weight, and inflammatory markers in women with PCOS. These early findings suggest that IF may improve insulin sensitivity, weight-related parameters, and inflammatory status, all of which are relevant to PCOS management. Still, due to limited and low-quality evidence, IF cannot yet be recommended as a therapeutic approach for PCOS until more rigorous, long-term clinical trials are conducted.
| Influence of IF on QoL and Circadian Rhythms | ▴Top |
In addition to improving hormonal and metabolic markers, IF also enhances circadian rhythms and QoL. One possible non-pharmacological treatment for PCOS is IF. However, further research is still needed to determine how it directly affects the QoL of women with PCOS. Although there are not many direct studies that only look at QoL, some studies have included QoL assessments as secondary outcomes. For example, one study that examined the effects of time-restricted eating on overweight and obese women with PCOS evaluated the 6-month effects of TRF on a number of parameters, including health-related QoL, in these women. In a study by Liu et al, participants followed an eating window from 8:00 a.m. to 4:00 p.m. in order to assess changes in weight, metabolic health, reproductive function, and QoL. However, there were few QoL findings [57]. The circadian rhythm is a biological clock that runs on a 24-h cycle and controls a number of physiological functions, including hormone production, body temperature, sleep-wake cycles, digestion, and metabolism. In women with PCOS, IF, particularly TRF, may have a beneficial effect on circadian rhythms, potentially enhancing hormonal and metabolic health [58]. IF may improve insulin sensitivity, better glucose regulation, and enhance sleep quality [59].
Heydari et al (2025) investigated the relationship between circadian rhythm disruption and PCOS by a systematic review and meta-analysis of the two conditions. The study evidence provided that women with PCOS exhibit significant alternations in circadian biomarkers such as melatonin levels, cortisol secretion, and sleep efficiency, compared to controls. These disruptions may contribute to the pathophysiology of PCOS [60].
A systematic review and meta-analysis of the effects of IF on female reproductive health, including its influence on circadian rhythms, was carried out by Mao et al in 2024 [42]. The review investigated how several IF regimens, such as the 5:2 diet, TRF, ADF, and Ramadan fasting, affected the reproductive function of females. With an emphasis on hormonal profiles, menstrual management, fertility, and pregnancy outcomes particularly in women with obesity or PCOS, it assessed data from both animal and human trials. By decreasing hyperandrogenism and increasing menstrual regularity, IF has the potential to improve reproductive function in obese and PCOS-afflicted women. However, care should be taken because of possible negative consequences in pregnant or healthy women. Before it is widely used in clinical settings, more thorough human research is necessary to ensure its safety and efficacy.
| Female Reproductive Function | ▴Top |
IF affects the functions in females in various ways depending on various factors such as fasting time and duration, caloric intake, nutritional status, stress management, and hormonal health. Female reproductive function is regulated by the hypothalamic-pituitary-ovarian (HPO) axis, a critical hormonal system that regulates female reproductive function. It involves a complex feedback loop between the brain and the ovaries, coordinating processes such as the menstrual cycle, ovulation, and fertility. This system involves release of GnRH by hypothalamus, LH, and estrogen hormone in response to GnRH by pituitary gland, estrogen and progesterone production by ovaries which regulates the menstrual cycle and ovulation [61]. IF regimens have been shown to increase SHBG concentrations in premenopausal females, particularly those with obesity and PCOS. This increase is more pronounced when most food is consumed in the morning or afternoon. For example, an 8-h TRE regimen increased SHBG levels in females with PCOS, and a 5:2 diet also led to a significant increase in SHBG in premenopausal women with obesity [61].
IF and CR provide significant health benefits, particularly for the cardiovascular and cerebrovascular systems. Both strategies enhance insulin sensitivity, and reduce blood pressure, heart rate, oxidative stress, and inflammation key risk factors for heart disease and stroke. They also increase heart rate variability and improve cardiovascular stress adaptation. CR and IF protect brain and heart cells from ischemic damage by promoting cellular stress resistance and reducing oxidative damage. These regimens enhance learning, memory, synaptic plasticity, and neurogenesis in animal tests, in part because they raise vascular endothelial growth factor (VEGF) and brain-derived neurotrophic factor (BDNF). The benefits of consistent exercise are reflected in these processes. Furthermore, age-related illnesses like diabetes, cancer, and neurodegeneration are postponed by both IF and CR, while extending lifespan in rodents and monkeys. The benefits apply to both obese and healthy individuals, although effects may be more pronounced in those with metabolic risk factors. Overall, IF and CR offer promising non-pharmacologic strategies for improving health span [62].
The effects of IF on female reproductive hormones vary; while some alterations in androgens and SHBG have been noted, other important hormones seem to be completely unaffected. In premenopausal women, especially those with obesity and PCOS, IF regimes, specifically TRE with early food consumption, have been demonstrated to lower androgen indicators like testosterone and the free androgen index (FAI). For example, in young women with PCOS and obesity, an 8-h TRE intervention (8 a.m. to 4 p.m.) dramatically decreased body weight by 2% and total testosterone and FAI levels. Similarly, in obese premenopausal women, a 5:2 diet significantly reduced FAI.
This reduction in androgens is considered beneficial for treating hyperandrogenic conditions like PCOS, which are characterized by high androgen levels leading to symptoms like hirsutism and menstrual cycle disorders. Lowering androgens can improve menstruation and fertility in these individuals.
IF has both positive and negative effects on female reproduction function.
A systematic review of the effects of IF on fertility was carried out by Velissariou et al [37]. This systematic review examined three major studies with an emphasis on PCOS and female reproductive outcomes. Of the participants, 33–73% reported improved or normalized menstrual cycles, and regularity was higher in groups using TRF combined with probiotics (up to 40%). Significant reductions were observed in total testosterone, FAI, SHBG, anti-Mullerian hormone (AMH), LH, FSH, and adrenal androgen levels. Metabolic and weight outcomes were improved like reduction in body weight, BMI, body fat %, visceral fat, IR, fasting insulin, and inflammatory markers (hs-CRP), and slight increase in insulin sensitivity which helps reduce hyperinsulinemia, a key PCOS mechanism. Therefore, TRF shows promising short-term benefits for improving fertility-related outcomes in women with PCOS, especially by reducing hyperandrogenism, enhancing menstrual cycle regularity, and improving insulin sensitivity.
Schroder et al conducted a study to assess the short-term effects of TRF in obese women, focusing on metabolic, hormonal, and anthropometric outcomes. TRF effectively reduced body weight and waist circumference (WC), a key marker of visceral fat and cardiovascular risk. However, no significant changes were observed in metabolic biomarkers like glucose, insulin, or cholesterol, possibly due to the high number of participants without metabolic syndrome (MetS) at baseline. The reduction in WC correlated positively with lower cardiovascular risk and body fat, and negatively with muscle mass, highlighting its value as a health indicator. Participants also reported improved QoL, likely linked to weight loss and better body image. TRF appears to be a practical dietary strategy for those unable to follow restrictive diets. While immediate metabolic changes were minimal, TRF remains a promising first-line intervention for managing obesity and associated health risks, warranting further long-term investigation [63].
As discussed earlier in this review, excessive adipose tissue can increase estrogen production and disrupt hormonal balance. Weight loss via IF can normalize and could improve cycle regularity. Chronic inflammations are generally associated with fertility issues, therefore IF may reduce inflammatory markers, and potentially support ovarian function [13]. In normal-weight or underweight women, or when fasting is extreme, IF can negatively impact reproductive function due to energy deficiency or stress. A potential negative effect of IF is hypothalamic amenorrhea (HA). IF, especially CR diet and low energy availability, can suppress GnRH release, leading to a drop in LH/FSH and ultimately amenorrhea (loss of menstruation). Chronic stress from fasting or under-eating increases cortisol, which can inhibit GnRH and suppress ovulation. Insufficient food intake can also reduce estrogen and progesterone production. Low estrogen levels over time can impair bone mineral density [64].
This review has several limitations. As a structured narrative review, it does not follow the formal methodology of a systematic review or meta-analysis, and therefore a comprehensive risk-of-bias assessment of included studies was not performed. Additionally, the available clinical evidence specifically evaluating IF in women with PCOS remains limited and heterogeneous in terms of study design, fasting protocols, and outcome measures. Consequently, conclusions of this review should be interpreted cautiously until larger randomized controlled trials are conducted.
| Evidence Hierarchy and Strength of Current Evidence | ▴Top |
The current body of evidence examining the role of IF in women with PCOS remains limited and heterogeneous. Most available clinical studies have focused primarily on metabolic outcomes such as weight reduction, insulin sensitivity, and lipid metabolism rather than direct endocrine outcomes. Improvements in IR, commonly measured using indices such as HOMA-IR, have been reported in several dietary intervention studies involving women with PCOS and in broader metabolic populations [65, 66].
Evidence suggesting improvements in reproductive hormonal parameters, including androgen levels, ovulatory function, and menstrual regularity, remains comparatively limited. Some clinical investigations and recent systematic reviews have suggested that IF or CR may contribute to improvements in metabolic parameters that indirectly influence androgen production and reproductive endocrine function in women with PCOS [67, 68]. However, the number of randomized clinical trials directly evaluating fasting protocols in PCOS populations remains small, and the heterogeneity in fasting regimens and study designs limits the ability to draw definitive conclusions.
Several mechanistic pathways discussed in this review including activation of AMPK, regulation of SIRT1 signaling, and inhibition of mTOR are supported primarily by experimental studies and metabolic research conducted in non-PCOS populations or animal models [69, 70]. These molecular mechanisms provide biological plausibility for the metabolic benefits associated with fasting, including improved insulin sensitivity, reduced oxidative stress, and modulation of inflammatory pathways.
While these findings offer important insights into the potential mechanisms linking IF with metabolic and endocrine regulation, their direct clinical applicability to women with PCOS remains to be fully established. Therefore, larger well-designed randomized controlled trials specifically investigating IF protocols in PCOS populations are needed to confirm the therapeutic potential of fasting-based dietary interventions.
| Conclusion | ▴Top |
Despite promising results, current research on IF in PCOS lacks long-term human studies and robust comparisons across IF protocols. Hormonal responses, particularly involving estrogen, LH, and FSH, remain inconsistently reported, and psychological outcomes are underexplored. Additionally, the role of circadian rhythm restoration in PCOS improvement is poorly understood, and differences in response based on weight status are unclear. Future studies should conduct long-duration randomized trials in diverse populations, investigate IF’s impact on the HPO axis, assess behavioral effects, and explore chrono nutrition strategies to establish IF as an effective and sustainable approach for managing PCOS.
IF represents a promising lifestyle-based intervention that may influence metabolic and hormonal pathways involved in PCOS. Current evidence suggests potential improvements in insulin sensitivity, metabolic flexibility, and inflammatory status, which may indirectly contribute to improved endocrine balance. However, direct clinical evidence evaluating hormonal outcomes in women with PCOS remains limited and heterogeneous. Future well-designed randomized controlled trials are required to establish the safety, efficacy, and optimal fasting protocols for different PCOS phenotypes.
Acknowledgments
The author thanks the SRM Medical College Hospital & Research Centre for their constant support and encouragement.
Financial Disclosure
The authors received no specific funding for this work.
Conflict of Interest
The authors declare that there are no conflicts of interest related to the content, authorship, or publication of this manuscript. No financial or non-financial interests have influenced the preparation or conclusions presented in this work.
Informed Consent
Not applicable. This manuscript does not contain any person’s data in any form (including individual details, images, or videos).
Author Contributions
UI: conceptualization, data curation, writing – original draft. MM and MG: supervision, writing – review & editing. All authors read and approved the final manuscript.
Data Availability
The datasets generated and/or analyzed during the current study are available in the publicly available sites.
| References | ▴Top |
- Cahill D. PCOS. BMJ Clin Evid. 2009;2009:1408.
pubmed - Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J Clin Endocrinol Metab. 1998;83(9):3078-3082.
doi pubmed - Teede H, Deeks A, Moran L. Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010;8:41.
doi pubmed - Jiang B. The global burden of polycystic ovary syndrome in women of reproductive age: findings from the GBD 2019 study. Int J Womens Health. 2025;17:153-165.
doi pubmed - Deswal R, Narwal V, Dang A, Pundir CS. The prevalence of polycystic ovary syndrome: a brief systematic review. J Hum Reprod Sci. 2020;13(4):261-271.
doi pubmed - Sharma A, Sarwal Y, Devi NK, Saraswathy KN. Polycystic Ovary Syndrome prevalence and associated sociodemographic risk factors: a study among young adults in Delhi NCR, India. Reprod Health. 2025;22(1):61.
doi pubmed - Siddiqui S, Mateen S, Ahmad R, Moin S. A brief insight into the etiology, genetics, and immunology of polycystic ovarian syndrome (PCOS). J Assist Reprod Genet. 2022;39(11):2439-2473.
doi pubmed - Christ JP, Cedars MI. Current guidelines for diagnosing PCOS. Diagnostics (Basel). 2023;13(6):1113.
doi pubmed - Kim KW. Unravelling polycystic ovary syndrome and its comorbidities. J Obes Metab Syndr. 2021;30(3):209-221.
doi pubmed - Su P, Chen C, Sun Y. Physiopathology of polycystic ovary syndrome in endocrinology, metabolism and inflammation. J Ovarian Res. 2025;18(1):34.
doi pubmed - Hoeger KM, Dokras A, Piltonen T. Update on PCOS: consequences, challenges, and guiding treatment. J Clin Endocrinol Metab. 2021;106(3):e1071-e1083.
doi pubmed - Rudnicka E, Suchta K, Grymowicz M, Calik-Ksepka A, Smolarczyk K, Duszewska AM, Smolarczyk R, et al. Chronic low grade inflammation in pathogenesis of PCOS. Int J Mol Sci. 2021;22(7):1-12.
doi pubmed - Islam H, Masud J, Islam YN, Haque FKM. An update on polycystic ovary syndrome: A review of the current state of knowledge in diagnosis, genetic etiology, and emerging treatment options. Womens Health (Lond). 2022;18:17455057221117966.
doi pubmed - Burger HG. Androgen production in women. Fertil Steril. 2002;77(Suppl 4):S3-S5.
doi pubmed - Qamar U, Atkin SL, Sathyapalan T. Obesity and polycystic ovary syndrome. Practical Guide to Obesity Medicine. 2017;3:59-70.
- Krug I, Giles S, Paganini C. Binge eating in patients with polycystic ovary syndrome: prevalence, causes, and management strategies. Neuropsychiatr Dis Treat. 2019;15:1273-1285.
doi pubmed - Alesi S, Ee C, Moran LJ, Rao V, Mousa A. Nutritional supplements and complementary therapies in polycystic ovary syndrome. Adv Nutr. 2022;13(4):1243-1266.
doi pubmed - Palomba S, Santagni S, Falbo A, La Sala GB. Complications and challenges associated with polycystic ovary syndrome: current perspectives. Int J Womens Health. 2015;7:745-763.
doi pubmed - Hussein RS, Dayel S Bin, Abahussein O. Polycystic ovary syndrome and reproductive health: a comprehensive review. Clin Exp Obstet Gynecol. 2024;51.
- Naderpoor N, Shorakae S, de Courten B, Misso ML, Moran LJ, Teede HJ. Metformin and lifestyle modification in polycystic ovary syndrome: systematic review and meta-analysis. Hum Reprod Update. 2015;21(5):560-574.
doi pubmed - Jungari M, Choudhary A, Gill NK. Comprehensive management of polycystic ovary syndrome: effect of pharmacotherapy, lifestyle modification, and enhanced adherence counseling. Cureus. 2023;15(2):e35415.
doi pubmed - Lim SS, Hutchison SK, Van Ryswyk E, Norman RJ, Teede HJ, Moran LJ. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2019;3(3):CD007506.
doi pubmed - Naka KK, Kalantaridou SN, Kravariti M, Bechlioulis A, Kazakos N, Calis KA, Makrigiannakis A, et al. Effect of the insulin sensitizers metformin and pioglitazone on endothelial function in young women with polycystic ovary syndrome: a prospective randomized study. Fertil Steril. 2011;95(1):203-209.
doi pubmed - Sadeghi HM, Adeli I, Calina D, Docea AO, Mousavi T, Daniali M, Nikfar S, et al. Polycystic ovary syndrome: a comprehensive review of pathogenesis, management, and drug repurposing. Int J Mol Sci. 2022;23(2).
doi pubmed - Gautam R, Maan P, Jyoti A, Kumar A, Malhotra N, Arora T. The role of lifestyle interventions in PCOS management: a systematic review. Nutrients. 2025;17(2):1-42.
doi pubmed - Jain A, Neravi A. Nutritional management of Polycystic Ovary Syndrome (PCOS) - a review. Biomed Pharmacol J. 2025;18(1):527-534.
doi - Feyzioglu BS, Guven CM, Avul Z. Eight-hour time-restricted feeding: a strong candidate diet protocol for first-line therapy in polycystic ovary syndrome. Nutrients. 2023;15(10):1-10.
doi pubmed - Salis S, Shefa S, Sharma N, Vora N, Anjana RM, Mohan V, et al. ORIGINAL ARTICLE effects of intermittent fasting on weight loss in Asian Indian adults with obesity. Journal of Association of Physicians of India. 2022;70:62-66.
- Obermayer A, Tripolt NJ, Pferschy PN, Kojzar H, Aziz F, Muller A, Schauer M, et al. Efficacy and safety of intermittent fasting in people with insulin-treated type 2 diabetes (INTERFAST-2)-a randomized controlled trial. Diabetes Care. 2023;46(2):463-468.
doi pubmed - Hoeger KM, Oberfield SE. Do women with PCOS have a unique predisposition to obesity? Fertil Steril. 2012;97(1):13-17.
doi pubmed - Teede HJ, Tay CT, Laven JJE, Dokras A, Moran LJ, Piltonen TT, Costello MF, et al. Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. J Clin Endocrinol Metab. 2023;108(10):2447-2469.
doi pubmed - Zafar MI, Mills KE, Zheng J, Regmi A, Hu SQ, Gou L, Chen LL. Low-glycemic index diets as an intervention for diabetes: a systematic review and meta-analysis. Am J Clin Nutr. 2019;110(4):891-902.
doi pubmed - Greenwell S, Jones A, Smith YR, Marriott D, Aikens JE, Padmanabhan V, Saslow LR. Protocol for a randomized comparative effectiveness trial comparing a very low-carbohydrate diet to DASH diet for polycystic ovary syndrome: the SUPER (Supporting Understanding of PCOS Education and Research) trial. Trials. 2024;25(1):750.
doi pubmed - Filippou C, Thomopoulos C, Konstantinidis D, Siafi E, Tatakis F, Manta E, Drogkaris S, et al. DASH vs. Mediterranean diet on a salt restriction background in adults with high normal blood pressure or grade 1 hypertension: a randomized controlled trial. Clin Nutr. 2023;42(10):1807-1816.
doi pubmed - Papadopoulou SK, Nikolaidis PT. Low-carbohydrate diet and human health. Nutrients. 2023;15(8):2004.
- Dynka D, Kowalcze K, Charuta A, Paziewska A. The ketogenic diet and cardiovascular diseases. Nutrients. 2023;15(15).
doi pubmed - Velissariou M, Athanasiadou CR, Diamanti A, Lykeridou A, Sarantaki A. The impact of intermittent fasting on fertility: A focus on polycystic ovary syndrome and reproductive outcomes in Women-A systematic review. Metabol Open. 2025;25:100341.
doi pubmed - Han Y, Lin B, Lu W, Wang X, Tang W, Tao X, Cai H, et al. Time-restricted feeding improves metabolic and endocrine profiles in mice with polycystic ovary syndrome. Front Endocrinol (Lausanne). 2022;13:1057376.
doi pubmed - Li C, Xing C, Zhang J, Zhao H, Shi W, He B. Eight-hour time-restricted feeding improves endocrine and metabolic profiles in women with anovulatory polycystic ovary syndrome. J Transl Med. 2021;19(1):148.
doi pubmed - Kalam F, Akasheh RT, Cienfuegos S, Ankireddy A, Gabel K, Ezpeleta M, Lin S, et al. Effect of time-restricted eating on sex hormone levels in premenopausal and postmenopausal females. Obesity (Silver Spring). 2023;31(Suppl 1):57-62.
doi pubmed - Kim JJ. Obesity and polycystic ovary syndrome. J Obes Metab Syndr. 2024;33(4):289-301.
doi pubmed - Mao L, Liu A, Zhang X. Effects of Intermittent Fasting on Female Reproductive Function: A Review of Animal and Human Studies. Curr Nutr Rep. 2024;13(4):786-799.
doi pubmed - Rojas J, Chavez M, Olivar L, Rojas M, Morillo J, Mejias J, Calvo M, et al. Polycystic ovary syndrome, insulin resistance, and obesity: navigating the pathophysiologic labyrinth. Int J Reprod Med. 2014;2014:719050.
doi pubmed - Manuscript A. insulin resistance and ovarian dysfunction. 2013;77:300-305.
- Escobar-Morreale HF, Luque-Ramirez M, Gonzalez F. Circulating inflammatory markers in polycystic ovary syndrome: a systematic review and metaanalysis. Fertil Steril. 2011;95(3):1048-1058 e1041-1042.
doi pubmed - Randeva HS, Tan BK, Weickert MO, Lois K, Nestler JE, Sattar N, Lehnert H. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33(5):812-841.
doi pubmed - Che T, Yan C, Tian D, Zhang X, Liu X, Wu Z. Time-restricted feeding improves blood glucose and insulin sensitivity in overweight patients with type 2 diabetes: a randomised controlled trial. Nutr Metab (Lond). 2021;18(1):88.
doi pubmed - Yuliyanasari N, Rejeki PS, Hidayati HB, Subsomwong P, Miftahussurur M. The effect of intermittent fasting on preventing obesity-related early aging from a molecular and cellular perspective. J Med Life. 2024;17(3):261-272.
doi pubmed - Access Open. We are IntechOpen, the world’s leading publisher of Open Access books Built by scientists, for scientists TOP 1% AMP-Activated Protein Kinase.
- Wu QJ, Zhang TN, Chen HH, Yu XF, Lv JL, Liu YY, Liu YS, et al. The sirtuin family in health and disease. Signal Transduct Target Ther. 2022;7(1):402.
doi pubmed - Sears B, Saha AK. Dietary control of inflammation and resolution. Front Nutr. 2021;8:709435.
doi pubmed - Heinonen T, Ciarlo E, Rigoni E, Regina J, Le Roy D, Roger T. Dual deletion of the sirtuins SIRT2 and SIRT3 impacts on metabolism and inflammatory responses of macrophages and protects from endotoxemia. Front Immunol. 2019;10:2713.
doi pubmed - Bunney PE, Zink AN, Holm AA, Billington CJ, Kotz CM. Orexin activation counteracts decreases in nonexercise activity thermogenesis (NEAT) caused by high-fat diet. Physiol Behav. 2017;176:139-148.
doi pubmed - Trepanowski JF, Kroeger CM, Barnosky A, Klempel MC, Bhutani S, Hoddy KK, Gabel K, et al. Effect of alternate-day fasting on weight loss, weight maintenance, and cardioprotection among metabolically healthy obese adults: a randomized clinical trial. JAMA Intern Med. 2017;177(7):930-938.
doi pubmed - Floyd R, Gryson R, Mockler D, Gibney J, Duggan SN, Behan LA. The effect of time-restricted eating on insulin levels and insulin sensitivity in patients with polycystic ovarian syndrome: a systematic review. Int J Endocrinol. 2022;2022:2830545.
doi pubmed - Gray KL, Clifton PM, Keogh JB. The effect of intermittent energy restriction on weight loss and diabetes risk markers in women with a history of gestational diabetes: a 12-month randomized control trial. Am J Clin Nutr. 2021;114(2):794-803.
doi pubmed - Liu H, Shangguan F, Liu F, Guo Y, Yu H, Li H, Su Y, et al. Evaluating the effects of time-restricted eating on overweight and obese women with polycystic ovary syndrome: A randomized controlled trial study protocol. PLoS One. 2025;20(1):e0316333.
doi pubmed - Gnocchi D, Bruscalupi G. Circadian rhythms and hormonal homeostasis: pathophysiological implications. Biology (Basel). 2017;6(1).
doi pubmed - Wang F, Xie N, Wu Y, Zhang Q, Zhu Y, Dai M, Zhou J, et al. Association between circadian rhythm disruption and polycystic ovary syndrome. Fertil Steril. 2021;115(3):771-781.
doi pubmed - Heydari T, Ramdass P. Circadian rhythm disruption and polycystic ovary syndrome: a systematic review and meta-analysis. AJOG Glob Rep. 2025;5(2):100479.
doi pubmed - Cienfuegos S, Corapi S, Gabel K, Ezpeleta M, Kalam F, Lin S, Pavlou V, et al. Effect of intermittent fasting on reproductive hormone levels in females and males: a review of human trials. Nutrients. 2022;14(11).
doi pubmed - Mattson MP, Wan R. Beneficial effects of intermittent fasting and caloric restriction on the cardiovascular and cerebrovascular systems. J Nutr Biochem. 2005;16(3):129-137.
doi pubmed - Schroder JD, Falqueto H, Manica A, Zanini D, de Oliveira T, de Sa CA, Cardoso AM, et al. Effects of time-restricted feeding in weight loss, metabolic syndrome and cardiovascular risk in obese women. J Transl Med. 2021;19(1):3.
doi pubmed - Song DK, Kim YW. Beneficial effects of intermittent fasting: a narrative review. J Yeungnam Med Sci. 2023;40(1):4-11.
doi pubmed - Tinsley GM, La Bounty PM. Effects of intermittent fasting on body composition and clinical health markers in humans. Nutr Rev. 2015;73(10):661-674.
doi pubmed - Anton SD, Moehl K, Donahoo WT, Marosi K, Lee SA, Mainous AG, 3rd, Leeuwenburgh C, et al. Flipping the metabolic switch: understanding and applying the health benefits of fasting. Obesity (Silver Spring). 2018;26(2):254-268.
doi pubmed - Harvie M, Howell A. Potential benefits and harms of intermittent energy restriction and intermittent fasting amongst obese, overweight and normal weight subjects-a narrative review of human and animal evidence. Behav Sci (Basel). 2017;7(1).
doi pubmed - Kalsekar AS, Abdelrahim DN, Faris ME. Effect of calorie restriction and intermittent fasting on glucose homeostasis, lipid profile, inflammatory, and hormonal markers in patients with polycystic ovary syndrome: a systematic review. Front Nutr. 2024;11:1362226.
doi pubmed - Longo VD, Mattson MP. Fasting: molecular mechanisms and clinical applications. Cell Metab. 2014;19(2):181-192.
doi pubmed - Mattson MP, Longo VD, Harvie M. Impact of intermittent fasting on health and disease processes. Ageing Res Rev. 2017;39:46-58.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.