| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Original Article
Volume 000, Number 000, May 2026, pages 000-000

Therapeutic Outcomes of Methimazole in Hyperthyroidism Patients
Raed Al-Dahasha, b, c, k, Mohammad Almarzoqid, Fahad Alenazib, Ahmed Alibrahimb, k, Saud Alrabaha, Abdulrahman Aljohanie, Saud Alsadhanf, Abdullah Alguraibig, Majed Almutairih, Sultan Athuwaybii, Abdularahman Alsaberj
aKing Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
bDepartment of Medicine, King Abdulaziz Medical City, Riyadh, Saudi Arabia
cKing Abdullah International Medical Research Center, Riyadh, Saudi Arabia
dDepartment of Medicine, King Fahad Medical City, Riyadh, Saudi Arabia
eDepartment of Radiology, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia
fDepartment of Pediatrics, King Abdullah Specialized Children’s Hospital, Riyadh, Saudi Arabia
gDepartment of Urology, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia
hDepartment of Medicine, King Salman Medical City, Riyadh, Saudi Arabia
iDepartment of Anesthesia, King Abdulaziz Medical City, Riyadh, Saudi Arabia
jDepartment of Orthopedics, King Salman Medical City, Riyadh, Saudi Arabia
kCorresponding Authors: Raed Al-Dahash, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; Ahmed Alibrahim, Department of Medicine, King Abdulaziz Medical City, Riyadh, Saudi Arabia
Manuscript submitted February 10, 2026, accepted April 17, 2026, published online May 27, 2026
Short title: Methimazole in Hyperthyroidism Patients
doi: https://doi.org/10.14740/jem1602
| Abstract | ▴Top |
Background: Hyperthyroidism is a disorder characterized by excessive thyroid hormone production. Methimazole is widely considered the first-line treatment due to its efficacy and favorable safety profile. However, there is limited contemporary local data on its clinical outcomes and adverse effects in Saudi Arabia. The aim of the study was to evaluate the efficacy and adverse effect profile of methimazole in adult patients with hyperthyroidism across varying treatment durations.
Methods: This retrospective case-crossover study was conducted at King Abdullah Specialized Children’s Hospital (KASCH). A total of 277 adult patients diagnosed with hyperthyroidism and treated with methimazole between January 2015, and December 2022 were included. Data were collected through chart review and analyzed using SAS version 9.4. A P value < 0.05 was considered statistically significant.
Results: The majority of patients were female (70.4%) and had Graves’ disease (71.5%). Treatment duration ranged from less than 6 months to more than 24 months. Gastrointestinal adverse effects, particularly sore throat, were significantly associated with longer treatment duration (P = 0.0067). Other adverse effects included dermatological reactions (30% rash), musculoskeletal symptoms (18.1% arthralgia), and hematological abnormalities (16.2% leukopenia), none of which showed significant variation across treatment durations. Older age was significantly associated with increased rates of anemia (P = 0.0340) and thrombocytopenia (P = 0.0019). Biochemical response was achieved in the majority of patients, with normalization of thyroid-stimulating hormone (TSH) in 73.7% and thyroxine (T4) in 55.5% of cases; however, a substantial proportion demonstrated low T4 levels post-treatment, suggesting potential overtreatment.
Conclusions: Methimazole is an effective and generally well-tolerated treatment for hyperthyroidism. However, prolonged therapy and older age are associated with an increased risk of adverse effects. These findings highlight the importance of individualized dose titration and regular monitoring to optimize treatment outcomes and minimize complications.
Keywords: Hyperthyroidism; Methimazole; Antithyroid drugs; Adverse effects; Thyroid function
| Introduction | ▴Top |
Hyperthyroidism is a disorder characterized by excessive synthesis and secretion of thyroid hormones, which ultimately leads to thyrotoxicosis, the clinical state in which symptoms become apparent [1, 2]. It represents a significant global health burden, with an estimated prevalence of 2–3% worldwide [3]. In Saudi Arabia, the prevalence of hyperthyroidism varies by sex, with an overall estimate of approximately 2.8% based on a large population sample [4].
Saudi Arabia is generally considered an iodine-sufficient country; therefore, Graves’ disease remains the leading cause of hyperthyroidism. However, other etiologies, including multinodular goiter, toxic adenoma, and iodine-induced hyperthyroidism, also contribute to disease burden [1, 4]. Importantly, iodine exposure from medications or iodinated contrast agents is not uncommon and may precipitate or exacerbate thyrotoxicosis, particularly in patients with autonomous thyroid nodules such as toxic adenoma [5, 6]. This highlights the need to consider iodine status and exposure when evaluating disease course and treatment response.
The management of hyperthyroidism includes both symptomatic and definitive pharmacological approaches [2]. Symptomatic treatment involves the use of beta-blockers to control manifestations such as palpitations, tremor, anxiety, and heat intolerance [7], as well as glucocorticoids in selected cases of ophthalmopathy and dermopathy [2]. Definitive medical therapy primarily relies on antithyroid drugs, namely methimazole and propylthiouracil (PTU), which constitute the mainstay of treatment [8]. These agents act by inhibiting thyroid peroxidase (TPO), thereby blocking the iodination of tyrosine residues and the coupling reactions required for thyroid hormone synthesis [8].
Methimazole is generally preferred due to its greater potency, longer half-life, and more favorable safety profile [9]. Carbimazole, commonly used in some regions including Saudi Arabia, is a prodrug that is rapidly converted to methimazole, the active compound [10]. However, PTU remains indicated in specific clinical scenarios, such as early pregnancy due to its lower teratogenic risk, and in thyroid storm because of its additional effect of inhibiting peripheral conversion of thyroxine (T4) to triiodothyronine (T3) [9]. Despite their efficacy, antithyroid drugs are associated with a range of adverse effects, including pruritus, rash, urticaria, arthralgia, arthritis, fever, altered taste sensation, nausea, and vomiting [11]. More serious complications include bone marrow suppression, which may result in agranulocytosis and anemia, as well as hepatotoxicity [11–13]. Notably, methimazole-associated hematological toxicity is dose-dependent, whereas PTU-related adverse effects may occur irrespective of dose and are associated with a higher risk of severe hepatotoxicity [14].
The efficacy and safety of methimazole are influenced by multiple factors, including dosage, treatment duration, underlying etiology of thyrotoxicosis, and patient-specific characteristics [9, 15]. For example, Graves’ disease, an autoimmune condition, typically requires longer-duration therapy, whereas in toxic adenoma or multinodular goiter, antithyroid drugs are often used as a short-term measure prior to definitive treatment such as surgery or radioiodine therapy [2]. This underscores the importance of individualized treatment strategies rather than fixed-duration regimens [16].
Relapse following methimazole therapy remains a significant clinical concern. Reported relapse rates range from 30–40% within the first year of therapy, increasing to 50–60% with longer treatment duration [17]. Additionally, recurrence rates of approximately 15% have been observed within 48 months following withdrawal after prolonged therapy (60–120 months), compared to higher rates of up to 53% following conventional treatment durations of 18–24 months [18]. These findings highlight the complexity of long-term disease control and the need for careful monitoring and dose titration to avoid both relapse and overtreatment, including iatrogenic hypothyroidism.
Despite the global body of evidence, local data from Saudi Arabia remain limited. The most recent study, published in 2001, reported a modest success rate of 11% with an average treatment duration of 9 months in a cohort of 100 patients [18]. Given the evolving understanding of disease management, as well as regional variations in iodine exposure and clinical practice, there is a clear need for updated real-world data. Therefore, the aim of this study is to address this gap by evaluating the therapeutic outcomes and safety profile of methimazole in a Saudi population, with particular emphasis on patient characteristics, treatment duration, and adverse effects, to inform more individualized and evidence-based clinical management.
| Materials and Methods | ▴Top |
Study population
This retrospective case-crossover study was conducted at King Abdullah Specialized Children’s Hospital (KASCH). Despite the institutional setting, the study focused exclusively on adult patients aged ≥ 18 years who were diagnosed with hyperthyroidism and treated with methimazole.
Inclusion criteria comprised patients aged ≥ 18 years with a confirmed diagnosis of hyperthyroidism who received methimazole therapy. Exclusion criteria included patients younger than 18 years, those who underwent definitive treatment (radioiodine ablation or thyroidectomy), and those treated with PTU.
Sample size and study period
The study included a total of 277 patients and covered the period from January 2015 to December 2022.
Sampling technique
A non-probability consecutive sampling method was employed, whereby all eligible patients meeting the inclusion criteria during the study period were included to minimize selection bias.
Data collection
Data were collected through a structured retrospective chart review using NGHA’s BESTCARE 2.0 hospital information system. Extracted data were recorded in a standardized Excel spreadsheet to ensure consistency. Baseline variables included demographic and clinical characteristics such as age, sex, body mass index (BMI), smoking status, alcohol consumption, and comorbidities (hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease, and coronary artery disease). Disease-specific variables included the type (etiology) of hyperthyroidism, date of diagnosis, and duration of methimazole therapy.
Given the known influence of disease etiology and iodine exposure on treatment response, hyperthyroidism was categorized into Graves’ disease, toxic adenoma, multinodular goiter, and other causes where documented. Primary outcomes included both efficacy and safety endpoints. Efficacy was assessed based on documented relapse of hyperthyroidism. Safety outcomes included dermatological (rash, pruritus, urticaria), musculoskeletal (arthralgia, arthritis), systemic (fever), gastrointestinal (nausea, vomiting, altered taste sensation), hematological (anemia), and hepatic (hepatotoxicity) adverse events. Where available, laboratory parameters (e.g., thyroid function tests and hematological indices) were reviewed; however, incomplete or missing data were noted and addressed in the analysis as a limitation inherent to retrospective study designs.
Exposure variables
Methimazole treatment duration was recorded and categorized into predefined intervals. Although these categories were used for comparative analysis, treatment duration was also considered as a continuous variable in exploratory analyses to better assess temporal trends in adverse events. Information on dosing regimens and medication adherence was limited due to the retrospective nature of the study and variability in documentation.
Data analysis
Participants were stratified based on age groups, etiology of hyperthyroidism, and duration of methimazole therapy. Categorical variables were summarized as frequencies and percentages. Continuous variables were assessed for normality and presented as mean ± standard deviation for normally distributed data or median with interquartile range for non-normally distributed data. Comparisons between groups were performed using the Chi-square test or Fisher’s exact test for categorical variables, and independent sample t-tests, one-way analysis of variance (ANOVA), or Kruskal–Wallis tests for continuous variables, as appropriate. A two-sided P value of < 0.05 was considered statistically significant. All statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Institutional Review Board (IRB) approval
This study was approved by the IRB of King Abdullah International Medical Research Center, Riyadh, Saudi Arabia (Protocol No. NRC23R/123/03).
Ethical compliance with human study
The study was conducted in compliance with the ethical standards of the responsible institution for human subjects and in accordance with the Declaration of Helsinki.
| Results | ▴Top |
Baseline characteristics
A total of 277 patients were included in the study (Table 1). The majority were female (n = 195, 70.4%), while males accounted for 29.6% (n = 82). Most patients were aged 30–59 years (n = 172, 62.1%), followed by those older than 59 years (n = 82, 29.6%), and a smaller proportion aged 18–29 years (n = 23, 8.3%).
 Click to view | Table 1. Baseline Demographic and Clinical Characteristics of the Study Population |
Regarding BMI, 2.2% (n = 6) were underweight, 19.1% (n = 53) had normal BMI, 32.5% (n = 90) were overweight, and 45.9% (n = 127) were classified as obese (BMI ≥ 30). Most patients were non-smokers (n = 246, 90.4%), while 9.6% (n = 26) were smokers.
As shown in Figure 1 and Table 1, Graves’ disease was the predominant etiology (n = 196, 71.5%), followed by toxic multinodular goiter or nodular disease (n = 48, 17.5%). Other causes included subclinical hyperthyroidism (n = 12, 4.4%), thyroiditis (n = 6, 2.2%), and unknown etiology (n = 12, 4.4%).
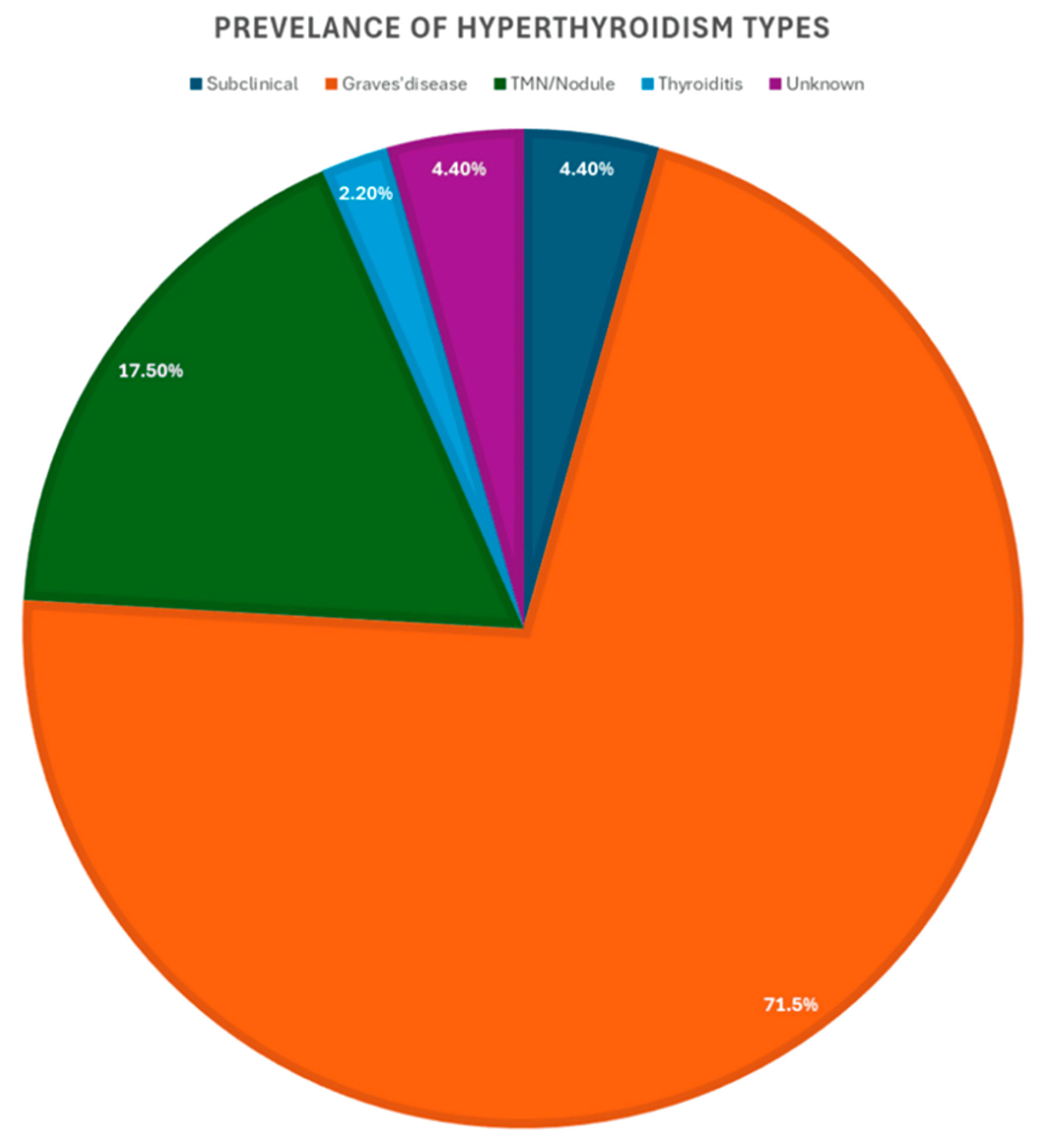 Click for large image | Figure 1. Prevalence of hyperthyroidism types. |
Methimazole treatment duration and adverse effects
Patients were categorized into four groups based on treatment duration: 0–6 months (n = 65), 6.1–12 months (n = 38), 12.1–24 months (n = 42), and > 24 months (n = 132) (Table 2). Gastrointestinal adverse effects were commonly reported. Sore throat occurred in 16.2% of patients (n = 44) and was significantly more frequent among those treated for more than 24 months (23.8%, P = 0.0067). Nausea (12.5%, n = 34) and vomiting (12.1%, n = 33) did not show statistically significant differences across treatment duration groups (P = 0.4334 and P = 0.1434, respectively). Hepatotoxicity was rare (2.2%, n = 6) and not associated with treatment duration (P = 1.0000).
Click to view | Table 2. Association Between Duration of Methimazole Therapy and Adverse Effects |
Musculoskeletal effects, primarily arthralgia, were observed in 18.1% of patients (n = 50), with no significant variation across treatment duration (P = 0.1962). Dermatological adverse effects included rash in 30% of patients (n = 83) and angioedema in 5.5% (n = 15), with no statistically significant differences between groups (P = 0.4737 and P = 0.7948, respectively). Hematological adverse effects included leukopenia (16.2%, n = 44), anemia (4.0%, n = 11), thrombocytopenia (7.3%, n = 20), and neutropenia (10.7%, n = 29), none of which demonstrated statistically significant associations with treatment duration (Table 2).
Age-stratified analysis of adverse effects
Patients were stratified into three age groups: 18–29 years (n = 23), 30–59 years (n = 172), and > 59 years (n = 82) (Table 3). Gastrointestinal adverse effects, including sore throat (16.2%), nausea (12.5%), vomiting (12.1%), and hepatotoxicity (2.2%), did not differ significantly across age groups. Similarly, arthralgia (18.1%) and rash (30%) showed no statistically significant variation.
Click to view | Table 3. Age-Stratified Distribution of Methimazole-Associated Adverse Effects |
However, certain adverse effects demonstrated significant associations with age. Angioedema was significantly more frequent in older patients (P = 0.0317). Hematological complications, including anemia (P = 0.0340) and thrombocytopenia (P = 0.0019), were also significantly more common in patients aged > 59 years. Leukopenia and neutropenia did not show statistically significant differences across age groups.
Adverse effects by etiology of hyperthyroidism
Patients were categorized by hyperthyroidism etiology into subclinical hyperthyroidism, Graves’ disease, toxic multinodular/nodular goiter, thyroiditis, and unknown causes (Table 4). Across all systems, most adverse effects did not significantly differ by disease etiology. Gastrointestinal symptoms, including sore throat, nausea, vomiting, and hepatotoxicity, showed no statistically significant variation. Similarly, musculoskeletal (arthralgia) and dermatological effects (rash) were not significantly associated with the underlying etiology. Angioedema demonstrated borderline statistical significance (P = 0.0521), while hematological effects, including leukopenia, anemia, thrombocytopenia, and neutropenia, were not significantly associated with hyperthyroidism type (Table 4).
Click to view | Table 4. Adverse Effects of Methimazole According to Etiology of Hyperthyroidism |
Thyroid function before and after methimazole therapy
Baseline thyroid function tests (Table 5) showed that the majority of patients had elevated T4 levels (> 12 µg/dL) prior to treatment (82.4%, n = 225), while 12.8% (n = 35) had values within the normal range and 0.4% (n = 1) had low levels. TSH levels were suppressed (< 0.35 µg/dL) in 84.4% (n = 233) of patients. Missing baseline data were noted for a small proportion of patients (T4: 4.4%, TSH: 3.6%). Following methimazole therapy, T4 levels normalized (5–12 µg/dL) in 55.5% of patients (n = 151), while 43.0% (n = 117) had levels below the normal range, suggesting possible overtreatment. Only 1.5% (n = 4) remained with elevated T4 levels. TSH levels normalized in 73.7% (n = 202) of patients, while 15.0% (n = 41) remained suppressed and 10.9% (n = 30) were elevated. Missing post-treatment TSH data were minimal (0.4%).
Click to view | Table 5. Thyroid Function Parameters (T4 and TSH) Before and After Methimazole Therapy |
| Discussion | ▴Top |
Methimazole remains a cornerstone in the management of hyperthyroidism, particularly in patients with Graves’ disease and, to a lesser extent, toxic multinodular goiter. In the present study, we evaluated the clinical outcomes, adverse effects, and biochemical response associated with methimazole therapy across different treatment durations, age groups, and etiologies. Overall, our findings are consistent with the existing literature, while also highlighting clinically relevant observations with important implications for individualized patient management. A comparative study found that long-term methimazole therapy resulted in a higher likelihood of maintaining euthyroidism than radioiodine treatment, which is often associated with persistent hypothyroidism [18]. This observation is consistent with our findings and highlights the importance of close monitoring in patients undergoing prolonged methimazole treatment.
A key finding of this study is that prolonged methimazole therapy (> 24 months) was associated with an increased incidence of certain adverse effects, particularly gastrointestinal symptoms such as sore throat (P = 0.0067). This observation aligns with previous reports suggesting that adverse events may accumulate over time, even though methimazole remains generally well tolerated [19]. However, it is important to note that methimazole toxicity is known to be dose-dependent [13]. Due to the retrospective nature of our study and inconsistent documentation of dosing regimens, we were unable to stratify adverse effects according to cumulative or daily dose. This represents an important limitation and may partially explain the observed associations between treatment duration and adverse events.
Dermatological adverse effects, particularly rash (30%), were among the most frequently observed in our cohort, consistent with prior studies [14]. Similarly, musculoskeletal symptoms such as arthralgia were observed in 18.1% of patients, which is in line with previously reported estimates of 15–20% [20]. These findings reinforce the well-established safety profile of methimazole, in which mild-to-moderate adverse effects are relatively common but rarely necessitate treatment discontinuation.
Hematological adverse effects, including leukopenia (16.2%), anemia (4.0%), and thrombocytopenia (7.3%), were also observed. While no significant association with treatment duration was identified, age-stratified analysis revealed that older patients were at significantly higher risk of anemia (P = 0.0340) and thrombocytopenia (P = 0.0019). This finding is clinically important and consistent with previous literature suggesting increased susceptibility to hematological toxicity in older individuals, possibly due to altered pharmacokinetics and reduced physiological reserve [20]. These results support the need for closer hematological monitoring in elderly patients receiving methimazole.
Another important observation is the high proportion of patients with low post-treatment T4 levels (43%), suggesting potential overtreatment. This finding raises concerns regarding inadequate dose titration and highlights the importance of regular biochemical monitoring and individualized dose adjustment. Rather than adhering to fixed treatment durations, our findings support a “titration-to-target” approach, where methimazole dosing is adjusted based on thyroid function tests to avoid both persistent hyperthyroidism and iatrogenic hypothyroidism. This is particularly relevant in real-world settings, where variability in follow-up practices may contribute to suboptimal outcomes.
The biochemical efficacy observed in this study further supports the role of methimazole as an effective therapy. TSH normalization was achieved in 73.7% of patients, while T4 normalization occurred in 55.5%, findings that are comparable to previously reported remission rates ranging from 50% to 80% [18, 21]. These outcomes underscore the importance of treatment adherence and early biochemical response as predictors of long-term remission.
Importantly, the underlying etiology of hyperthyroidism must be considered when interpreting treatment outcomes. Graves’ disease, which accounted for the majority of cases in our cohort, is an autoimmune condition that often requires prolonged therapy to achieve remission. In contrast, toxic adenoma and multinodular goiter represent autonomous thyroid activity, where antithyroid drugs are typically used as a temporary measure prior to definitive treatment such as radioiodine therapy or surgery. The lack of significant differences in adverse effects across etiological subgroups in our study may reflect the relatively small sample sizes in non-Graves’ categories, as well as the absence of stratification by treatment intent.
In this context, recent advances in thyroid diagnostics, including the application of artificial intelligence (AI) in cytopathology, have shown promise in improving the accuracy and standardization of thyroid nodule evaluation, particularly in indeterminate cases. AI-based approaches can analyze complex cytological patterns and may enhance diagnostic precision beyond conventional methods, although further validation is required before routine clinical implementation [22]. In addition, certain histopathological findings, such as psammoma bodies, may further complicate diagnostic interpretation. While typically associated with papillary thyroid carcinoma, the presence of psammoma bodies in the absence of an identifiable tumor poses a diagnostic challenge and may necessitate extensive evaluation to exclude occult malignancy. Although rare, their occurrence in benign conditions has also been reported, underscoring the importance of careful pathological assessment and clinical correlation [23].
These approaches are supported by established international guidelines, including the American Thyroid Association (ATA) recommendations, which provide evidence-based guidance on diagnosis, risk stratification, and management of thyroid disorders [6].
In addition, iodine exposure represents an important but often underrecognized factor influencing both disease activity and treatment response. Although Saudi Arabia is generally considered iodine-sufficient, exposure to iodine-containing medications or contrast agents may precipitate or exacerbate thyrotoxicosis, particularly in patients with nodular thyroid disease. This may contribute to variability in treatment response and highlights the need for clinicians to account for iodine exposure when managing hyperthyroid patients.
When compared to alternative treatment modalities, methimazole continues to demonstrate a favorable benefit-risk profile. Studies have shown that methimazole is associated with higher rates of euthyroidism compared to radioiodine therapy, which more commonly results in permanent hypothyroidism [18, 24]. Furthermore, radioiodine therapy has been linked to an increased risk of Graves’ ophthalmopathy [25], while methimazole offers a reversible and titratable treatment option.
For patients who are unable to tolerate methimazole, PTU remains an alternative, although it is associated with a higher risk of severe adverse effects, including hepatotoxicity and vasculitis [26]. Nevertheless, PTU remains the treatment of choice in specific clinical scenarios, such as the first trimester of pregnancy, due to the teratogenic potential of methimazole [27]. In rare cases of severe methimazole intolerance, alternative strategies such as lithium or early definitive therapy may be considered, as previously reported [28].
Strengths and limitations
This study has several notable strengths. It provides real-world clinical data on methimazole use in a relatively large cohort from Saudi Arabia, a region where contemporary data on hyperthyroidism management remain limited. The inclusion of diverse patient subgroups, stratified by age, treatment duration, and etiology of hyperthyroidism, allowed for a comprehensive evaluation of factors influencing both efficacy and adverse effects. Additionally, the study offers clinically relevant insights into age-related differences in hematological toxicity and highlights patterns of potential overtreatment, which are often underreported in routine clinical practice.
However, several limitations should be considered. First, the retrospective design inherently introduces the possibility of incomplete or inconsistent data recording, particularly for key variables such as thyroid function tests (TSH and T4) and medication dosing. The lack of detailed information on methimazole dosing regimens and patient adherence limits the ability to fully assess dose-dependent toxicity, which is a critical aspect of antithyroid drug safety. Second, the categorization of treatment duration into predefined intervals, rather than employing time-to-event analyses, may have reduced the sensitivity to detect temporal relationships between drug exposure and adverse outcomes. Third, the relatively small sample sizes in certain subgroups, particularly non-Graves’ etiologies, may have limited the ability to detect statistically significant differences. Finally, potential confounders such as iodine exposure (e.g., contrast agents or medications) were not systematically captured, which may influence both disease course and treatment response.
Clinical implications
The findings of this study have several important clinical implications. First, the observed association between older age and increased risk of hematological adverse effects underscores the need for age-specific monitoring strategies, including more frequent complete blood count assessments in elderly patients receiving methimazole.
Second, the high proportion of patients with low post-treatment T4 levels suggests a risk of overtreatment, emphasizing the importance of individualized dose titration rather than reliance on fixed treatment durations. Regular monitoring of thyroid function tests and timely dose adjustments are essential to maintain euthyroidism and avoid iatrogenic hypothyroidism.
Third, the lack of significant differences in adverse effects across treatment durations and etiologies highlights the importance of tailoring treatment strategies based not only on duration but also on the underlying cause of hyperthyroidism. For instance, patients with Graves’ disease may benefit from longer-term immunomodulatory therapy, whereas those with toxic adenoma or multinodular goiter should be considered for definitive treatment once euthyroidism is achieved.
Furthermore, clinicians should remain vigilant regarding potential iodine exposure, particularly in iodine-sufficient regions, as this may alter disease activity and influence treatment response.
Overall, these findings support a more individualized, patient-centered approach to methimazole therapy, incorporating factors such as age, etiology, biochemical response, and risk of adverse effects to optimize outcomes.
Conclusions
In conclusion, this study supports the continued use of methimazole as an effective and generally well-tolerated treatment for hyperthyroidism. While most adverse effects are mild, the risk of hematological complications appears to increase with age, underscoring the importance of age-specific monitoring strategies. The findings also highlight the potential for overtreatment, emphasizing the need for individualized dose titration and regular biochemical follow-up rather than reliance on fixed treatment durations. Consideration of disease etiology and iodine exposure is essential for optimizing therapeutic outcomes. Future research should focus on prospective, dose-stratified analyses and standardized monitoring approaches to further refine methimazole treatment strategies and improve patient outcomes.
Acknowledgments
The authors have no acknowledgments to declare.
Financial Disclosure
The authors declare that there was no financial support or funding for this study.
Conflict of Interest
The authors declare that they have no conflicts of interest.
Informed Consent
Not applicable.
Author Contributions
Dr. Raed Al-Dahash (Principal Investigator) conceptualized and supervised the study. Dr. Ahmed Alibrahim (co-corresponding author) contributed to study design and manuscript revision. Mohammad Almarzoqi and Fahad Alenazi were responsible for data collection and analysis. Ahmed Alibrahim and Saud Alrabah contributed to methodology development and interpretation of results. Abdulrahman Aljohani and Saud Alsadhan assisted with data curation and literature review. Abdullah Alguraibi and Majed Almutairi contributed to manuscript drafting and editing. Sultan Athuwaybi and Abdularahman Alsaber provided clinical input and critical revision of the manuscript. All authors reviewed and approved the final version of the manuscript.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Lee SY, Pearce EN. Hyperthyroidism: a review. JAMA. 2023;330(15):1472-1483.
doi pubmed - Wiersinga WM, Poppe KG, Effraimidis G. Hyperthyroidism: aetiology, pathogenesis, diagnosis, management, complications, and prognosis. Lancet Diabetes Endocrinol. 2023;11(4):282-298.
doi pubmed - Graves’ Disease. 2023. Accessed January 12. National Organization: https://rarediseases.org/rare-diseases/graves-disease/.
- Qashqary M, Tobaiqy M, Al-Sutari MM, Mujallad A, Alsheikh I. Prevalence of suspected cases of hyperthyroidism in Jeddah by using Wayne's Scoring Index. Cureus. 2020;12(11):e11538.
doi pubmed - Grani G, Sponziello M, Filetti S, Durante C. Thyroid nodules: diagnosis and management. Nat Rev Endocrinol. 2024;20(12):715-728.
doi pubmed - Ringel MD, Sosa JA, Baloch Z, Bischoff L, Bloom G, Brent GA, Brock PL, et al. 2025 American Thyroid Association Management Guidelines for adult patients with differentiated thyroid cancer. Thyroid. 2025;35(8):841-985.
doi pubmed - Szybiak-Skora W, Miedziaszczyk M, Szalek E, Lacka K. The therapeutic potential of propranolol and other beta-blockers in hyperthyroidism. Int J Mol Sci. 2025;26(17):8322.
doi pubmed - Haxhihyseni D, Krasniqi M, Kalaja R. Graves' ophthalmopathy: a comprehensive review of current evidence and management approaches. Interdisciplinary Journal of Research and Development. 2023;10(1):17.
- Liu Y, Li Q, Xu Y, Chen Y, Men Y. Comparison of the safety between propylthiouracil and methimazole with hyperthyroidism in pregnancy: a systematic review and meta-analysis. PLoS One. 2023;18(5):e0286097.
doi pubmed - Singh SK, et al. Effect of low and high doses of carbimazole in the treatment of Grave’s thyrotoxicosis: a prospective, open-label, and observational study. Thyroid Research and Practice. 2025;21(2):66-71.
- Arai M, Tsuno T, Konishi H, Nishiyama K, Terauchi Y, Inoue R, Shirakawa J. A disproportionality analysis of the adverse effect profiles of methimazole and propylthiouracil in patients with hyperthyroidism using the Japanese adverse drug event report database. Thyroid. 2023;33(7):804-816.
doi pubmed - Ramirez Stieben LA, Brun LR, Nasazzi Doddi P, Brance ML. Antithyroid drugs and the dose-risk balance: a meta-analysis on agranulocytosis in hyperthyroidism. Endocrine. 2025;90(2):391-403.
doi pubmed - He Q, Li M, Ji P, Zheng A, Yao L, Zhu X, Shin JG, et al. Comparison of drug-induced liver injury risk between propylthiouracil and methimazole: a quantitative systems toxicology approach. Toxicol Appl Pharmacol. 2024;491:117064.
doi pubmed - Sun Y, Wang S, Zhou X. Adverse events of the thyroid peroxidase inhibitor methimazole in the treatment of hyperthyroidism: a comprehensive analysis from the first quarter of 2004 to the first quarter of 2025. Front Endocrinol (Lausanne). 2025;16:1680281.
doi pubmed - Tan S, Chen L, Jin L, Fu X. The efficiency and safety of methimazole and propylthiouracil in hyperthyroidism: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2021;100(30):e26707.
doi pubmed - Chowdhury R, et al. Approach to hyperthyroidism. Journal of Otorhinolaryngology, Hearing and Balance Medicine. 2024;5(2):20.
- Wang PW. Prediction of relapse after antithyroid drugs withdrawal: a narrative review. 2020.
- Azizi F, Amouzegar A, Tohidi M, Hedayati M, Khalili D, Cheraghi L, Mehrabi Y, et al. Increased remission rates after long-term methimazole therapy in patients with Graves' disease: results of a randomized clinical trial. Thyroid. 2019;29(9):1192-1200.
doi pubmed - Azizi F, Abdi H, Cheraghi L, Amouzegar A. Treatment of subclinical hyperthyroidism in the elderly: comparison of radioiodine and long-term methimazole treatment. Thyroid. 2021;31(4):545-551.
doi pubmed - Azizi F, Saadat N, Takyar MA, Abdi H, Mehran L, Amouzegar A. Efficacy and safety of long-term methimazole versus radioactive iodine in the treatment of toxic multinodular goiter. Endocrinol Metab (Seoul). 2022;37(6):861-869.
doi pubmed - Azizi F, Takyar M, Madreseh E, Amouzegar A. Long-term methimazole therapy in Juvenile Graves' disease: a randomized trial. Pediatrics. 2019;143(5):e20183034.
doi pubmed - Fiorentino V, et al. The minefield of indeterminate thyroid nodules: could artificial intelligence be a suitable diagnostic tool? Diagnostic Histopathology. 2023;29(8):396-401.
- Cardisciani L, Policardo F, Tralongo P, Fiorentino V, Rossi ED. What psammoma bodies can represent in the thyroid. What we recently learnt from a story of lack of evidence. Pathologica. 2022;114(5):373-375.
doi pubmed - Abd-ElGawad M, et al. Efficacy of methimazole versus radioiodine in patients with hyperthyroidism: a meta-analysis of randomized controlled trials. 2023.
- Quah NQX, Sobti MM, Wren AM, Scawn R, Kalogianni E, Cleland J, Maenhout A. Radioactive iodine treatment for Graves' hyperthyroidism: incidence of Graves orbitopathy. Nucl Med Commun. 2024;45(2):103-107.
doi pubmed - Khan I, Okosieme O, Lazarus J. Antithyroid drug therapy in pregnancy: a review of guideline recommendations. Expert Rev Endocrinol Metab. 2017;12(4):269-278.
doi pubmed - Miao Y, Xu Y, Teng P, Wang A, Zhang Y, Zhou Y, Liu W. Efficacy of propylthiouracil in the treatment of pregnancy with hyperthyroidism and its effect on pregnancy outcomes: A meta-analysis. PLoS One. 2022;17(3):e0265085.
doi pubmed - VanCleave T, Kellis A, Oktaei H. The use of lithium to manage hyperthyroidism in the setting of methimazole induced agranulocytosis. The American Journal of the Medical Sciences. 2026;371:S133-S134.
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.