| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://jem.elmerpub.com |
Original Article
Volume 16, Number 3, June 2026, pages 157-165

Long-Term Postsurgical Hypoparathyroidism: Subtle Musculoskeletal Alterations and Marked Quality-of-Life Impairment
Elif Seray Korkmaza, d ![]() , Serife Mehlika Kuskonmazb, Cagatay Emir Onderb, Cevriye Mulkogluc, Esma Cecelic, Cavit Culhab
, Serife Mehlika Kuskonmazb, Cagatay Emir Onderb, Cevriye Mulkogluc, Esma Cecelic, Cavit Culhab
aDepartment of Endocrinology and Metabolism, Osmangazi University, Eskisehir, Turkey
bDepartment of Endocrinology and Metabolism, Ankara Education and Research Hospital, Ankara, Turkey
cDepartment of Physical Therapy and Rehabilitation, Ankara Education and Research Hospital, Ankara, Turkey
dCorresponding Author: Elif Seray Korkmaz, Department of Endocrinology and Metabolism, Osmangazi University, Eskisehir, Turkey
Manuscript submitted December 2, 2025, accepted February 12, 2026, published online June 10, 2026
Short title: Long-Term Postsurgical HypoPT
doi: https://doi.org/10.14740/jem1607
| Abstract | ▴Top |
Background: Postsurgical hypoparathyroidism (hypoPT) is associated with hypocalcemia and musculoskeletal complaints, yet its long-term impact on muscle function and quality of life remains poorly defined. This study aimed to evaluate muscle function, physical performance, and quality of life in patients with long-standing postsurgical hypoPT, in comparison with individuals with hypothyroidism (hypoT) and healthy controls.
Methods: The study included 90 participants: 30 with postsurgical hypoparathyroidism and hypothyroidism (hypoPT + T), 30 with postsurgical hypothyroidism alone (hypoT), and 30 healthy controls. Muscle strength was evaluated using BIODEX concentric isokinetic dynamometry and handgrip testing. Functional performance was assessed with the timed up and go (TUG) and repeated chair stand (RCS) tests. Body composition was measured by bioimpedance analysis, and quality of life was evaluated using the short form questionnaire-36 version 2 (SF-36v2) and World Health Organization Five Welfare Index questionnaire (WHO-5) questionnaires.
Results: Fat-free mass (FFM) was lower in the hypoPT + T group compared with controls (P < 0.01), although objective muscle strength did not differ significantly between groups. HypoPT + T patients exhibited prolonged TUG and RCS times and significantly lower SF-36v2 physical function scores (P < 0.01) compared with both hypoT patients and controls. WHO-5 scores were also reduced in the hypoPT + T group (P < 0.01), indicating impaired well-being independent of hypoT.
Conclusions: Long-standing postsurgical hypoPT is associated with impaired functional performance and reduced quality of life, despite preserved objective muscle strength. These findings highlight the need for management strategies that address patient-reported outcomes and physical function, beyond conventional biochemical control.
Keywords: Hypoparathyroidism; Hypothyroidism; Muscle strength; Quality of life
| Introduction | ▴Top |
Hypoparathyroidism (hypoPT) is an endocrine disorder characterized by decreased serum calcium and increased serum phosphorus due to parathyroid hormone (PTH) deficiency. In adults, the most common etiology is neck surgery [1]. The acute manifestations of hypoPT result from hypocalcemia and may range from mild symptoms to epileptic seizures, heart failure, and laryngeal spasm [2, 3]. In the chronic phase, renal and cardiac complications, basal ganglia calcifications, cataracts, dental abnormalities, and ectodermal manifestations may occur [2]. Although myopathy associated with severe hypocalcemia has been reported in case studies [4–10], patients with hypoPT frequently experience impaired quality of life (QoL) and persistent musculoskeletal complaints even when serum calcium is maintained within the recommended range through active vitamin D analogues and calcium supplementation [10].
Despite these observations, data on the long-term impact of hypoPT on muscle function remain limited. Therefore, in this study, we aimed to assess muscle function and QoL in patients with postsurgical hypoPT and hypoT, and to compare these findings with those of patients with postsurgical hypoT alone and with healthy controls.
| Materials and Methods | ▴Top |
Study subjects
This study was planned and carried out according to a prospective methodological approach. Written informed consent was obtained from all participants after they were informed about the purpose, methods, potential risks, and benefits of the study prior to enrollment.
We included 30 patients with postoperative hypoPT (hypoPT + T group); 30 patients with postoperative hypoT (hypoT group), and 30 age- and sex-matched healthy volunteers.
We defined hypoPT + T as an inappropriately low plasma PTH concentration in the presence of hypocalcemia, requiring continuous treatment with an active vitamin D analogue (alphacalcidol or calcitriol) or high-dose ergocalciferol (vitamin D2) for at least 12 months. At the time of inclusion, participants were required to have stable plasma ionized calcium (Ca2+) levels within, or slightly below, the lower limit of the reference interval, with no recent episodes of either hypocalcemia or hypercalcemia.
Patients with hypoT were included only if they had been on continuous levothyroxine (LT4) therapy for at least 2 years prior to inclusion and were matched with hypoPT + T patients in terms of age, gender, and timing of surgery.
The control group consisted of healthy volunteers presenting to the internal medicine outpatient clinic who had no identified chronic medical conditions.
A detailed informed consent was obtained from all participants. All participants underwent a general physical and neuromuscular examination including height and weight measurements. Body fat distribution was measured using a bioimpedance device (TANITA model TBF-300). Patients with a history of malignant disease, patients with chronic liver or kidney disease, neuromuscular disease or disabilities, pregnant or lactating women are not involved in the study.
Our study was approved by the ethics committee (EPK) of Health Sciences on 30.04.2019/E-19 and was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Biochemical evaluation
Plasma thyroid-stimulating hormone (TSH), free thyroxine (fT4), albumin, calcium, phosphate, magnesium, creatinine, creatinine kinase (CK), PTH, and 25-hydroxy vitamin D (25OHD) levels were measured biochemically (Roche Cobas 8000, Roche Cobas 6000).
The estimated glomerular filtration rate (GFR) was calculated by the CKD-EPI formula [11]. In order to avoid the effects of muscle function tests on the plasma levels of measured indices, care was taken to take blood samples before testing muscle function. To reduce analytical diversity, plasma PTH and 25OHD plasma levels were analyzed in a single batch.
QoL
Short form questionnaire-36 version 2 (SF-36v2) and World Health Organization Five Welfare Index questionnaire (WHO-5) were applied to the participants. SF-36v2 survey consists of 36 questions in eight subgroups: physical function, physical limitations, emotional well-being, emotional limitation, energy, social function, body pain, and general health perception. Total score is calculated for each subscale. Points are obtained in the range of 0–100; the higher the score, the better the QoL [12].
The WHO-5 questionnaire consists of five questions that evaluate the emotional well-being of patients. Answers to WHO-5 questions are scored from 0 (worst) to 5 (best). The raw score is multiplied by 4 to get a percentage score between 0 and 100. Zero percent represents the worst possible QoL, while 100% represents the best possible QoL. A score of 50% or less shows that the person does not feel emotionally well; a score of 28% or less indicates that advanced examination is required for depression [13].
Muscle strength
Jamar hand dynamometer recommended by the American Hand Therapists Association and accepted as the gold standard in many studies was used in order to measure the handgrip strength to evaluate muscle strength to the upper extremity [14]. Finger pinchmeter was used to measure fine grip force such as hand finger pinch grip, lateral grip, and triple grip force. Patients were measured in the sitting position, shoulder adduction and neutral rotation, elbow 90° flexion, forearm in neutral position and supported, on the hand side of the wrist that was actively used, with the wrist in neutral. During the test, 3 min were taken between each measurement for hand grip and finger grip strengths, and averages were recorded [15, 16]. Measurements were recorded in kilograms (kg).
Concentric isokinetic muscle strength of the lower extremities was assessed using a BIODEX concentric isokinetic dynamometer (Biodex Medical Systems, Shirley, NY, USA) during knee extension and flexion at angular velocities of 60°/s, 120°/s, and 180°/s. Peak torque is the measurement at the highest muscle strength output at any time during repetition [17]. It shows the capacity of muscle strength. Peak torque is the measurement with the least measurement error and the highest reliability and specificity among the concentric isokinetic force indices frequently used in scientific research [18].
Tests of muscle function
For the muscle function evaluation, the repeated chair stands (RCS) and timed up & go test (TUG) were applied to the participants.
In RCS, the patient was allowed to sit upright in the chair, with a seating height of 44 cm, and can sit back. The chair is fixed on the wall. He was then asked to stand up and sit without using hands from the chair for 30 s consecutively. It was recorded how many times he sat up in 30 s [19].
In TUG, the patient was seated upright in the chair. After telling the patient about the 3 m area in front of the chair, the patient was told to get up from the chair and walk this distance and sit again. Elapsed time was recorded in seconds [20].
Statistical analysis
The data were analyzed in IBM SPSS Statistics version of Windows 22.0 (IBM Corp., Armonk, New York, USA). The distribution of variables was checked with the Kolmogorov-Simirnov test. Average, standard deviation (SD), median, number of cases, and percentiles were used in the descriptive statistics of the data. Mann-Whitney U test was used to compare quantitative binary data, and Kruskal-Wallis test was used to analyze nonparametric quantitative triple data. Spearman correlation test was used to compare quantitative data with every other. Pearson Chi-square test and Fisher’s exact Chi-square tests were used to compare qualitative data.
| Results | ▴Top |
The demographic characteristics of the study groups are presented in Table 1. The groups were well matched with respect to age, sex, height, weight, and body mass index (BMI). Fat-free mass (FFM) differed significantly among the three groups (one-way analysis of variance (ANOVA), P = 0.01). Post-hoc analyses demonstrated that FFM was significantly lower in the hypoPT + T group compared with healthy controls (36.3 ± 14.3 vs. 44.7 ± 10.6 kg; P < 0.01). In contrast, no statistically significant difference in FFM was observed between the hypoPT + T and hypoT groups (36.3 ± 14.3 vs. 37.6 ± 14.4 kg; P > 0.01).
 Click to view | Table 1. Demographic Characteristics of Groups |
The type of thyroid surgery, time since surgery, and surgical indications were similar between the hypoT and hypoPT + T groups (Table 2).
Click to view | Table 2. Comparison of Thyroid Surgery Type, Time After Surgery, Diseases Necessitating Surgery of Groups |
Biochemical characteristics of the groups are summarized in Table 3. No significant differences were observed among the three groups in terms of TSH, fT4, creatinine, corrected calcium, phosphorus, magnesium, or 25-hydroxyvitamin D levels. As expected, PTH concentrations were significantly lower in the hypoPT + T group compared with the control group (P < 0.01). Although CK levels remained within the normal range, they were significantly higher in both the hypoPT + T and hypoT groups compared with controls (78.3 ± 41.8 vs. 116.5 ± 62.6 and 119.4 ± 57.2 U/L, respectively).
Click to view | Table 3. Biochemical Evaluation of the Participants |
There were no statistically significant differences among the groups in upper-extremity muscle strength parameters, including pinch grip, lateral grip, three-jaw chuck grip, and handgrip strength measurements (P > 0.01) (Table 4). Likewise, concentric isokinetic muscle strength (peak torque) of the lower extremities during knee extension and flexion at angular velocities of 60°/s, 120°/s, and 180°/s did not differ significantly between groups (P > 0.01) (Table 4).
Click to view | Table 4. Concentric Isokinetic Muscle Strength Measurements Assessed by BIODEX Dynamometry |
Functional performance tests demonstrated that the hypoPT + T group had lower RCS scores compared with controls (P < 0.01) and longer TUG completion times (P < 0.01) (Table 5). No significant differences were observed between the hypoPT + T and hypoT groups in either RCS or TUG results (P > 0.01). However, TUG times were significantly longer in the hypoT group compared with controls (P < 0.01).
Click to view | Table 5. TUG and RCS Test Results |
QoL outcomes assessed using the SF-36v2 questionnaire are shown in Figure 1. The hypoPT + T group scored significantly lower than controls on physical functioning, physical limitation, emotional limitation, vitality, social functioning, bodily pain, and general health perception (P < 0.01). No significant difference was observed between these two groups in emotional well-being. When compared with the hypoT group, the hypoPT + T group had significantly lower scores in physical functioning, pain, and general health perception (P < 0.01). Additionally, the hypoT group showed significantly lower vitality and general health perception scores compared with controls.
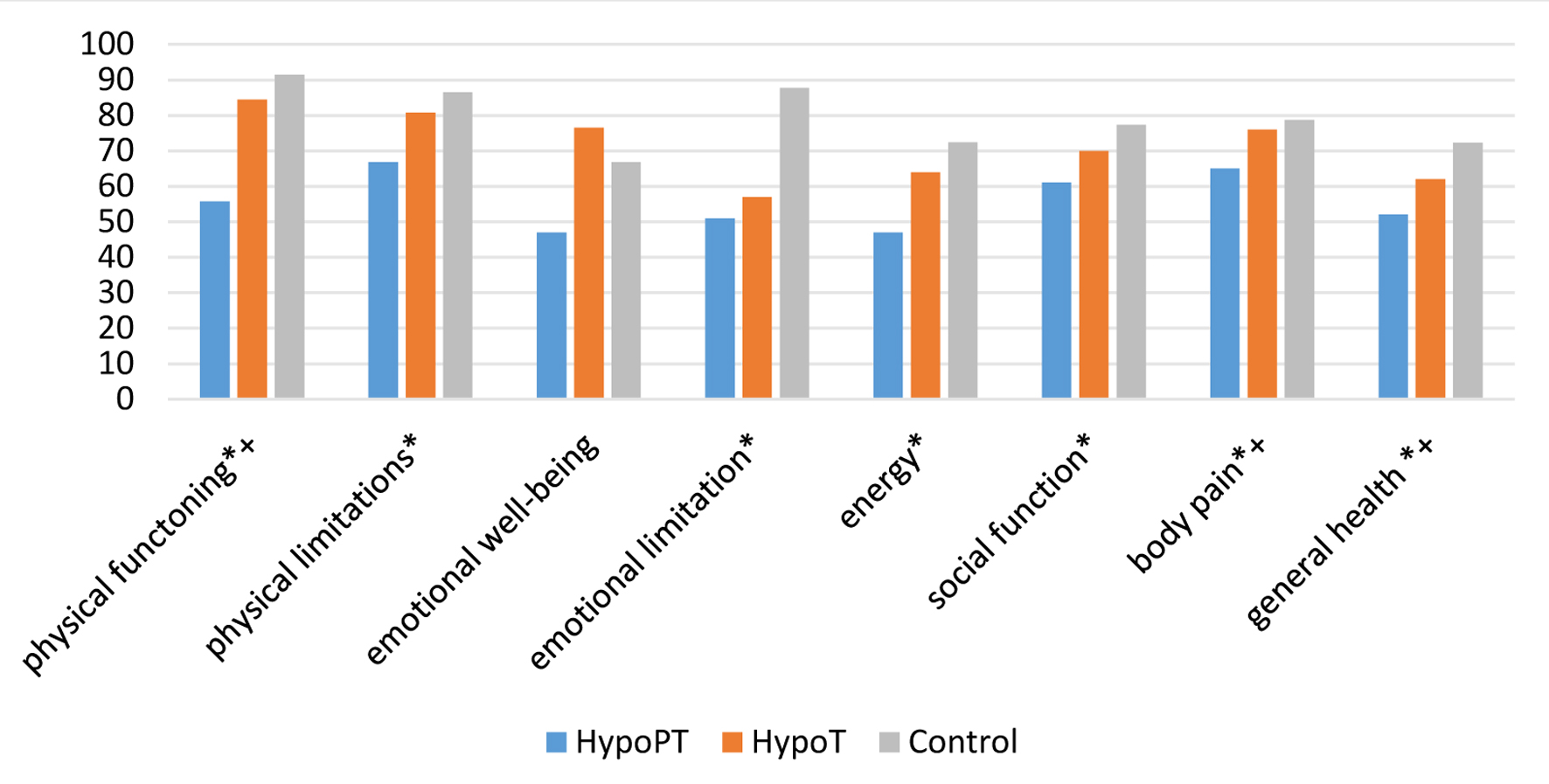 Click for large image | Figure 1. SF-36v2 domain scores in healthy controls, postsurgical hypothyroidism (hypoT), and postsurgical hypoparathyroidism with hypothyroidism (hypoPT + T). Data are presented as mean ± SD. **P < 0.01 vs. control group. †P < 0.05 vs. hypoT group. |
WHO-5 well-being index scores were significantly lower in the hypoPT + T group compared with both the hypoT and control groups (P < 0.01) (Fig. 2). In the hypoPT + T group, one participant (3.3%) scored below 28%, and 17 participants (56%) scored below 50%.
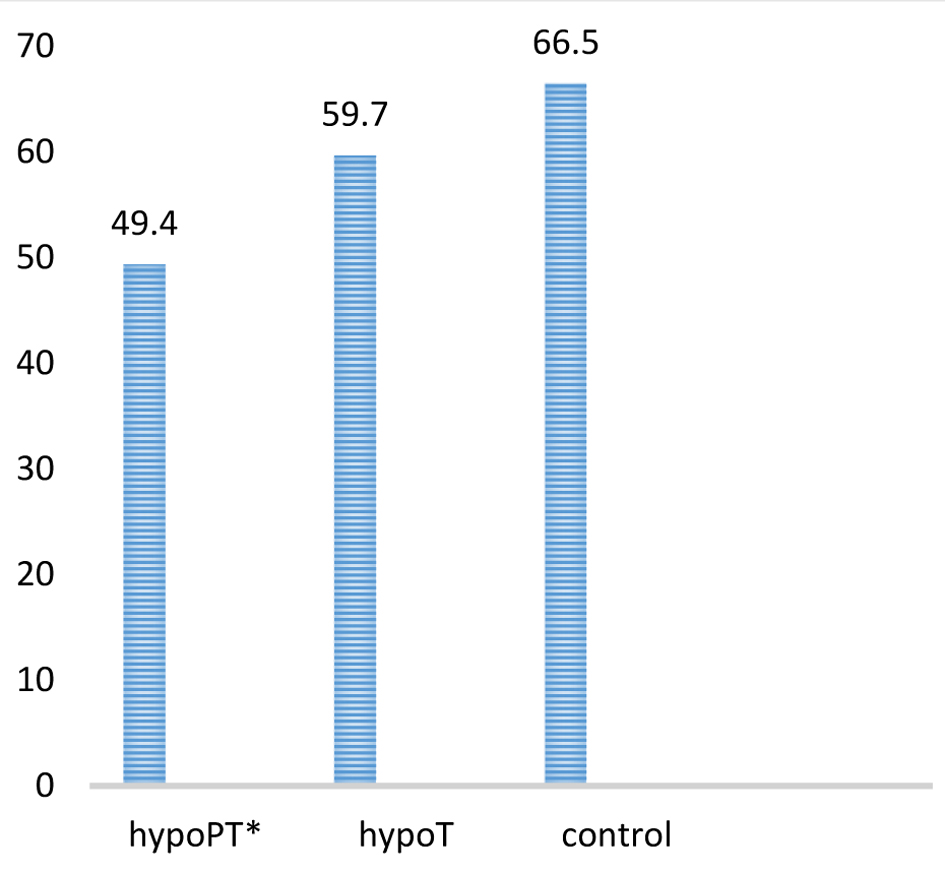 Click for large image | Figure 2. WHO-5 well-being index scores in healthy controls, postsurgical hypothyroidism (hypoT), and postsurgical hypoparathyroidism with hypothyroidism (hypoPT + T). Data are presented as mean ± SD. *P < 0.01 vs. control and hypoT groups. |
Overall, our findings indicate that despite largely preserved biochemical parameters and muscle strength measurements, patients with postsurgical hypoPT exhibit reduced functional performance and impaired QoL, suggesting subtle but clinically relevant musculoskeletal and psychosocial effects of chronic PTH deficiency.
| Discussion | ▴Top |
In this study, we comprehensively evaluated muscle strength, physical performance, and QoL in patients with postsurgical hypoPT + T with long-standing disease duration and compared them with appropriately matched hypothyroid and healthy control groups. Although patients with hypoPT + T are generally considered biochemically “well controlled” with current replacement strategies, our findings indicate that these patients continue to experience significant impairments in QoL despite largely preserved muscle strength.
Previous studies have reported that patients with postsurgical hypoPT + T experience musculoskeletal symptoms and reduced physical functioning even when hypocalcemia is adequately managed. Consistent with these observations, Sikjaer et al demonstrated reduced muscle strength in patients with hypoPT + T compared with both hypoT patients and healthy controls, despite relatively short disease duration (mean 2 years). In contrast, we did not observe significant reductions in concentric isokinetic muscle strength or handgrip strength in our hypoPT + T cohort. This discrepancy may be partly explained by the longer disease duration in our population (mean 8 years), which may provide a more stable representation of long-term adaptations in chronic hypoPT + T. Additionally, our study utilized highly standardized and validated measurement tools, including the BIODEX concentric isokinetic system and Jamar dynamometer, which may contribute to methodological differences between studies [21].
Previous research has demonstrated that assessing the concentric isokinetic performance of the knee extensors is a reliable and valid method for evaluating muscle strength [22]. Accordingly, in our study, we utilized the Biodex concentric isokinetic dynamometer to measure the concentric performance of the knee extensor muscles, enabling an objective and methodologically robust assessment of lower-limb muscle function.
In another study, 68% of patients with chronic hypoPT reported subjective muscle weakness, and a considerable proportion experienced functional limitations such as difficulty climbing stairs; importantly, these symptoms did not improve after 6 months of treatment with PTH (1–84), and no significant changes were detected in objective strength or physical performance measures [4].
In our study, serum CK levels were higher in hypoT and hypoPT + T groups compared with controls. This finding may be more closely related to concomitant hypoT rather than hypoPT itself. Indeed, Sikjaer and colleagues reported no significant differences in CK levels among hypoPT, hypoT, and control groups [23]. In contrast, CK elevation associated with hypoT has been frequently reported in the literature and shown to normalize following L-thyroxine replacement therapy [24, 25]. Marked CK elevation in hypoPT has predominantly been described in case reports involving severe hypocalcemia, in which non-specific histological changes on muscle biopsy have also been reported [25–28]. The biochemical stability of patients in our cohort may therefore explain why CK elevations were modest and not specific to hypoPT. Moreover, serum phosphate levels in the hypoPT + T group were only mildly elevated and did not differ significantly between groups, which may be related to stable biochemical control under treatment. Considering the proposed role of phosphate in neuromuscular dysfunction, the limited degree of hyperphosphatemia observed in our study appears insufficient to account for the functional impairments on its own.
In our study, QoL assessments revealed marked impairment in patients with hypoPT, despite preserved muscle strength, particularly in the physical functioning domains of the SF-36v2 and in overall well-being as measured by the WHO-5 index. These findings are consistent with previous studies demonstrating persistently reduced QoL in hypoPT despite conventional therapy [29–31]. Using data from the PARADIGHM™ registry, Clarke et al reported a high prevalence of fatigue, paresthesia, muscle twitching, and musculoskeletal pain in patients with chronic hypoPT, along with similarly reduced SF-36 physical component scores [32]. The reduction in QoL observed in our hypoT group appears to be independent of concomitant hypoT, as patients treated with LT4 generally exhibited substantially better physical functioning and well-being. Importantly, the fact that patients had serum calcium levels within the target range and were biochemically stable at the time of evaluation allowed QoL and functional outcomes to be assessed independently of acute electrolyte disturbances. This suggests that the observed impairment in QoL may reflect chronic effects of hypoPT rather than transient hypocalcemic episodes. Nevertheless, symptoms specific to hypoPT, such as muscle cramps, paresthesias, and neuromuscular irritability, were not systematically assessed in our study. These symptoms may contribute substantially to patient-perceived QoL impairment, independent of measurable muscle strength or functional performance, and should be considered in the interpretation of our findings.
FFM values measured by bioimpedance analysis were lower in the hypoPT + T group compared with healthy controls; however, the numerical difference between the hypoPT + T and hypoT groups was limited and characterized by substantial overlap. The relationship between the observed differences in FFM and hypoPT or concomitant hypoT should be interpreted cautiously in light of the available findings. Body composition was assessed using bioimpedance analysis, a practical and non-invasive method that is widely used in clinical studies and has been shown to provide reliable estimates of body composition, particularly in group-based comparisons [33, 34]. Nevertheless, bioimpedance-derived measurements are known to be influenced by hydration status and electrolyte distribution [35]. In hypoPT, subtle alterations in fluid distribution related to disturbances in calcium homeostasis, even if not clinically apparent, may have partially affected FFM estimates. In this regard, the lack of confirmation by dual-energy X-ray absorptiometry (DXA), which is considered a reference method for body composition assessment, can be regarded as an important limitation of the study [36]. To date, body composition in chronic hypoPT has not been comprehensively investigated, and no previous studies have directly compared FFM measurements in this patient population. As our study was not designed to test a predefined hypothesis regarding body composition, these findings highlight the need for further research to clarify whether chronic disturbances in mineral homeostasis contribute to changes in muscle mass.
As reported in previous similar studies, our study also demonstrated significant impairment in TUG and RCS test performance in the hypoPT + T group [4, 23]. These tests reflect not only muscle force generation but also integrated functional components, including neuromotor coordination, balance, endurance, and aspects of cognitive processing. Accordingly, impaired performance on TUG and RCS may indicate subtle neuromuscular or integrative functional deficits that are not captured by isolated measurements of muscle strength. This dissociation underscores the clinical importance of functional testing in hypoPT and supports the notion that patient-perceived physical limitations may arise independently of measurable muscle weakness.
Studies investigating the effects of recombinant PTH on QoL and functional outcomes in patients with hypoPT have yielded heterogeneous results. Cusano and colleagues reported early and marked improvements in SF-36 scores with PTH (1–84) therapy [8], while Palermo and colleagues observed sustained improvements, particularly in physical functioning and general health, with long-term PTH (1–34) treatment [37]. In contrast, randomized controlled trials conducted by Sikjaer and colleagues found that PTH (1–84) therapy did not confer significant benefits in SF-36 or WHO-5 scores, muscle strength, or functional performance tests (RCS and TUG) [4]. As no patients in our study were receiving PTH therapy, our findings reflect the QoL and functional status of patients with hypoPT managed with conventional treatment.
The pathophysiological mechanisms underlying impaired physical function despite preserved muscle strength remain incompletely understood. Although acute hypocalcemia is known to cause tetany and muscle dysfunction, patients included in our study were biochemically stable at the time of evaluation, and recent hypocalcemic or hypercalcemic episodes were excluded. Nevertheless, the absence of physiological PTH secretion may contribute to suboptimal intracellular calcium handling, impaired neuromuscular excitability, or cumulative effects of chronic hyperphosphatemia that are not reflected in standard strength measurements [1, 26]. These potential mechanisms warrant further investigation in future studies incorporating neuromuscular electrophysiological assessments and advanced imaging techniques.
Overall, our findings highlight that while long-standing postsurgical hypoPT + T may not be associated with measurable reductions in muscle strength, QoL remains significantly compromised, particularly in domains related to physical functioning. These results emphasize the need for treatment strategies that extend beyond biochemical correction to address patient-reported outcomes, and they underscore the importance of future research exploring the mechanisms linking chronic hypoPT + T to impaired well-being.
Conclusion
In patients with long-standing postsurgical hypoPT, we observed a clear dissociation between preserved objective muscle strength and impaired functional performance and QoL. Although FFM was modestly lower compared with healthy controls, this difference was not accompanied by proportional strength deficits and showed substantial overlap with the hypoT group. Despite comparable BIODEX concentric isokinetic and handgrip strength measurements, patients with hypoPT and concomitant hypothyroidism (hypoPT + T) demonstrated significantly poorer performance on the TUG and RCS tests, along with lower SF-36v2 physical functioning scores and reduced WHO-5 well-being.
These findings underscore the need for comprehensive management strategies in hypoPT + T that extend beyond biochemical correction to address patient-reported outcomes and functional performance, and highlight the importance of further longitudinal studies to elucidate the long-term musculoskeletal and neurocognitive consequences of this condition.
Strengths and limitations
Our study has several strengths, including a relatively large sample size compared with previous literature, strict group matching procedures, long disease duration, and the use of validated and objective muscle strength assessments, including the BIODEX concentric isokinetic dynamometer, which provides highly accurate and reproducible measurements. The comprehensive evaluation of muscle strength, functional performance, body composition, and QoL in a well-characterized cohort further strengthens the clinical relevance of our findings.
Nevertheless, several limitations should be acknowledged. Body composition was assessed using bioimpedance analysis rather than DXA, which is considered a reference method; thus, FFM estimates may have been influenced by hydration status and electrolyte balance. Nutritional factors and habitual physical activity levels, which may affect muscle mass and functional performance, were not systematically evaluated. In addition, symptoms commonly associated with hypoPT, such as muscle cramps, paresthesias, and neuromuscular irritability, were not formally assessed and may have contributed to impaired QoL independently of objective strength or functional measures. Although the study population reflects routine clinical practice, the cross-sectional design precludes causal inference.
Acknowledgments
None to declare.
Financial Disclosure
The authors declare that no financial support or funding was received from any institution or organization for this study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Written informed consent was obtained from all participants prior to their enrollment in the study.
Author Contributions
Conceptualization: Elif Seray Korkmaz, Serife Mehlika Kuskonmaz. Methodology: Elif Seray Korkmaz, Serife Mehlika Kuskonmaz, Cagatay Emir Onder. Data collection: Elif Seray Korkmaz, Cevriye Mulkoglu, Esma Ceceli. Formal analysis: Elif Seray Korkmaz. Writing – original draft: Elif Seray Korkmaz. Writing – review & editing: Elif Seray Korkmaz, Serife Mehlika Kuskonmaz, Cagatay Emir Onder. Supervision: Elif Seray Korkmaz, Serife Mehlika Kuskonmaz, Cavit Culha. All authors have read and approved the final manuscript.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
25OHD: 25-hydroxy vitamin D; Ca2+: ionized calcium; CK: creatine kinase; DXA: dual-energy X-ray absorptiometry; FFM: fat-free mass; fT4: free thyroxine; GFR: glomerular filtration rate; hypoPT + T: postsurgical hypoparathyroidism with hypothyroidism; hypoPT: hypoparathyroidism; hypoT: postsurgical hypothyroidism; LT4: levothyroxine; PTH: parathyroid hormone; RCS: repeated chair stands; SF-36v2: short form-36 version 2; TUG: timed up and go test; TSH: thyroid-stimulating hormone; WHO-5: World Health Organization Five Well-Being Index
| References | ▴Top |
- Bilezikian JP, Khan A, Potts JT, Jr., Brandi ML, Clarke BL, Shoback D, Juppner H, et al. Hypoparathyroidism in the adult: epidemiology, diagnosis, pathophysiology, target-organ involvement, treatment, and challenges for future research. J Bone Miner Res. 2011;26(10):2317-2337.
doi pubmed - Francesca G, Maria Luisa B. Clinical presentation of hypoparathyroidism. Parathyroid Disorders. 2019;51:139-146.
- Fong J, Khan A. Hypocalcemia: updates in diagnosis and management for primary care. Can Fam Physician. 2012;58(2):158-162.
pubmed - Sikjaer T, Rejnmark L, Rolighed L, Heickendorff L, Mosekilde L, Hypoparathyroid Study G. The effect of adding PTH(1-84) to conventional treatment of hypoparathyroidism: a randomized, placebo-controlled study. J Bone Miner Res. 2011;26(10):2358-2370.
doi pubmed - Arlt W, Fremerey C, Callies F, Reincke M, Schneider P, Timmermann W, Allolio B. Well-being, mood and calcium homeostasis in patients with hypoparathyroidism receiving standard treatment with calcium and vitamin D. Eur J Endocrinol. 2002;146(2):215-222.
doi pubmed - Santonati A, Palermo A, Maddaloni E, Bosco D, Spada A, Grimaldi F, Raggiunti B, et al. PTH(1-34) for surgical hypoparathyroidism: a prospective, open-label investigation of efficacy and quality of life. J Clin Endocrinol Metab. 2015;100(9):3590-3597.
doi pubmed - Abe S, Tojo K, Ichida K, Shigematsu T, Hasegawa T, Morita M, Sakai O. A rare case of idiopathic hypoparathyroidism with varied neurological manifestations. Intern Med. 1996;35(2):129-134.
doi pubmed - Cusano NE, Rubin MR, McMahon DJ, Irani D, Tulley A, Sliney J, Jr., Bilezikian JP. The effect of PTH(1-84) on quality of life in hypoparathyroidism. J Clin Endocrinol Metab. 2013;98(6):2356-2361.
doi pubmed - Brandi ML, Bilezikian JP, Shoback D, Bouillon R, Clarke BL, Thakker RV, Khan AA, et al. Management of Hypoparathyroidism: Summary Statement and Guidelines. J Clin Endocrinol Metab. 2016;101(6):2273-2283.
doi pubmed - Buttner M, Musholt TJ, Singer S. Quality of life in patients with hypoparathyroidism receiving standard treatment: a systematic review. Endocrine. 2017;58(1):14-20.
doi pubmed - Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, 3rd, Feldman HI, Kusek JW, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604-612.
doi pubmed - Hoare SR, Usdin TB. Molecular mechanisms of ligand recognition by parathyroid hormone 1 (PTH1) and PTH2 receptors. Curr Pharm Des. 2001;7(8):689-713.
doi pubmed - Ware JE, Kosinski M, Gandek B. SF-36 health survey: manual and interpretation guide. QualityMetric Incorporated; 2005.
- de Wit M, Pouwer F, Gemke RJ, Delemarre-van de Waal HA, Snoek FJ. Validation of the WHO-5 Well-Being Index in adolescents with type 1 diabetes. Diabetes Care. 2007;30(8):2003-2006.
doi pubmed - Shechtman O, Gestewitz L, Kimble C. Reliability and validity of the DynEx dynamometer. J Hand Ther. 2005;18(3):339-347.
doi pubmed - Haidar SG, Kumar D, Bassi RS, Deshmukh SC. Average versus maximum grip strength: which is more consistent? J Hand Surg Br. 2004;29(1):82-84.
doi pubmed - Halpern CA, Fernandez JE. The effect of wrist and arm postures on peak pinch strength. J Hum Ergol (Tokyo). 1996;25(2):115-130.
pubmed - Biodex Medical Systems. Biodex Rev 4.59. 2015.
- Rikli R, Jones J. Development and validation of a functional fitness test for community-residing adults. J Aging Phys Act. 1999;7:129-161.
- Podsiadlo D, Richardson S. The timed "Up & Go": a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142-148.
doi pubmed - Underbjerg L, Sikjaer T, Rejnmark L. Health-related quality of life in patients with nonsurgical hypoparathyroidism and pseudohypoparathyroidism. Clin Endocrinol (Oxf). 2018;88(6):838-847.
doi pubmed - Johnson J, Siegel D. Reliability of an isokinetic movement of the knee extensors. Res Q. 1978;49(1):88-90.
pubmed - Sikjaer T, Moser E, Rolighed L, Underbjerg L, Bislev LS, Mosekilde L, Rejnmark L. Concurrent hypoparathyroidism is associated with impaired physical function and quality of life in hypothyroidism. J Bone Miner Res. 2016;31(7):1440-1448.
doi pubmed - Burnett JR, Crooke MJ, Delahunt JW, Feek CM. Serum enzymes in hypothyroidism. N Z Med J. 1994;107(985):355-356.
pubmed - Syriou V, Kolitsa A, Pantazi L, Pikazis D. Hypoparathyroidism in a patient presenting with severe myopathy and skin rash. Case report and review of the literature. Hormones (Athens). 2005;4(3):161-164.
doi pubmed - Barber J, Butler RC, Davie MW, Sewry CA. Hypoparathyroidism presenting as myopathy with raised creatine kinase. Rheumatology (Oxford). 2001;40(12):1417-1418.
doi pubmed - Kurihara I. [Rhabdomyolysis in a patient with postoperative hypothyroidism and hypoparathyroidism]. Nihon Jinzo Gakkai Shi. 2008;50(1):59-63.
pubmed - Nora DB, Fricke D, Becker J, Gomes I. Hypocalcemic myopathy without tetany due to idiopathic hypoparathyroidism: case report. Arq Neuropsiquiatr. 2004;62(1):154-157.
doi pubmed - Rolighed L, Amstrup AK, Jakobsen NF, Sikjaer T, Mosekilde L, Christiansen P, Rejnmark L. Muscle function is impaired in patients with "asymptomatic" primary hyperparathyroidism. World J Surg. 2014;38(3):549-557.
doi pubmed - Rolighed L, Rejnmark L, Sikjaer T, Heickendorff L, Vestergaard P, Mosekilde L, Christiansen P. No beneficial effects of vitamin D supplementation on muscle function or quality of life in primary hyperparathyroidism: results from a randomized controlled trial. Eur J Endocrinol. 2015;172(5):609-617.
doi pubmed - Dai CL, Sun ZJ, Zhang X, Qiu MC. Elevated muscle enzymes and muscle biopsy in idiopathic hypoparathyroidism patients. J Endocrinol Invest. 2012;35(3):286-289.
doi pubmed - Clarke BL, Ing S, Khan A, Kearns A, Rejnmark L, Shoback D, et al. Chronic hypoparathyroidism disease profile from 492 patients in the PARADIGHM global registry. Endocrine Abstracts. 2017;49:EP291.
- Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Gomez JM, Heitmann BL, et al. Bioelectrical impedance analysis—part I: review of principles and methods. Clin Nutr. 2004;23(5):1226-1243.
doi pubmed - Kyle UG, Genton L, Slosman DO, Pichard C. Fat-free and fat mass percentiles in healthy subjects measured by bioelectrical impedance analysis. Clin Nutr. 2001;20:327-333.
- Earthman C, Traughber D, Dobratz J, Howell W. Bioimpedance spectroscopy for clinical assessment of fluid distribution and body cell mass. Nutr Clin Pract. 2007;22(4):389-405.
doi pubmed - Lee SY, Gallagher D. Assessment methods in human body composition. Curr Opin Clin Nutr Metab Care. 2008;11(5):566-572.
doi pubmed - Palermo A, Santonati A, Tabacco G, Bosco D, Spada A, Pedone C, Raggiunti B, et al. PTH(1-34) for surgical hypoparathyroidism: a 2-year prospective, open-label investigation of efficacy and quality of life. J Clin Endocrinol Metab. 2018;103(1):271-280.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.